The Psychological Implications of Concealing a Stigma: A Cognitive–Affective–Behavioral Model
Psychological Bulletin
| Volume | 133 |
| Issue | 2 |
| Pagination | 328–345 |
| Type of Work | Essay, Research |
| DOI | 10.1037/0033-2909.133.2.328 |
... A Cognitive–Affective–Behavioral Model
John E. Pachankis
Stony Brook University, State University of New York
- Remarks by Ipce:
This article mentions several examples of stigmas. In the field of sexuality, it mentions especially having HIV, having had an abortus and having not-heterosexual desires, as being gay.
Not mentioned, even in this article about stigma and secrets, is having pedophilic feelings and desires: clearly even here a taboo. Having this strong taboo in mind, the reader will learn how difficult it is if one has to hide that stigma, how many consequences it has for the psychic well-being of the person.
There are situations in which disclosure of the secret stigma, to trusted persons, may deminish the negative effects. Thus, dislosure of those feelings to trusted people may be helpful.
Fellow human beings might accept those feelings better if the feelings and desires keep being feelings and desires, thus do not lead or have lead to acts. May be these feelings may ever been accepted as human feelings.
Another important subject is the existence of a secret that must be kept hidden, a situation that has many complications and a negative influence of the well-being. Such a situation is also not mentioned here: the child or teenager that has had secret sexual experiences with an adult, an experience that must be kept hidden and thus negatively influences the young person. The reader might also have this situation in mind.
In the case of children and teenagers, it is doubtable that disclosure of the secret, maybe except to a therapist, will deminish the negative effects.
Thus, as is said already here above, it is better to avoid acts that would lead to the need to hide secrets, and thus to quite negative implications for the young fellow human being. Maybe ever, once in the future, openness in these cases will be possible.
[Abstract]
Many assume that individuals with a hidden stigma escape the difficulties faced by individuals with a visible stigma. However, recent research has shown that individuals with a concealable stigma also face considerable stressors and psychological challenges. The ambiguity of social situations combined with the threat of potential discovery makes possessing a concealable stigma a difficult predicament for many individuals.
The increasing amount of research on concealable stigmas necessitates a cohesive model for integrating relevant findings. This article offers a cognitive–affective–behavioral process model for understanding the psychological implications of concealing a stigma. It ends with discussion of potential points of intervention in the model as well as potential future routes for investigation of the model.
Keywords: stigma, conceal, secrecy, disclosure, self-evaluation
[Introduction]
In recent years, researchers have paid increasing attention to the experience of possessing a devalued trait that is obvious to others, such as being a member of a racially stigmatized group
- (Clark, Anderson, Clark, & Williams, 1999; Crocker, Major, & Steele, 1998; Dion, 2002; Dohrenwend, 2000; Kessler, Mickelson, & Williams, 1999; Kessler & Neighbors, 1986; Wethington & Kessler, 1986; Williams, Yu, Jackson, & Anderson, 1997).
Meanwhile, many have assumed that individuals with a concealable stigma (e.g., being gay) escape much of the prejudice and discrimination faced by visibly stigmatized individuals because they can hide their stigma (Goffman, 1963; Jones et al., 1984). However, individuals with concealable stigmas may also face considerable stressors. These include having to make decisions to disclose one’s hidden status, anxiously anticipating the possibility of being found out, being isolated from similarly stigmatized others, and being detached from one’s true self. Efforts to conceal a stigma can have a powerful, negative impact on an individual’s daily life.
Yet, until recently, very few psychologists have paid much attention to the unique experiences of individuals with a hidden stigma. This article reviews the research on the difficulties of concealing a stigma, highlights how these difficulties differ from those faced by individuals with a visible stigma, and offers an integrative model for understanding these findings.
Individuals with a concealable stigma face many challenges in choosing whether, when, how, and to whom to disclose their stigma
- (e.g., Derlega & Berg, 1987; K. Greene, Derlega, Yep, & Petronio, 2003; Holmes & River, 1998; Kelly & McKillop, 1996; Larson & Chastain, 1990).
Unlike individuals with a visible stigma, individuals with a concealable stigma must face disclosure decisions regularly. In every new situation that is encountered, such individuals must decide who among the present company knows of their stigma, who may suspect this stigma, and who has no suspicion of the stigma. The difficulty of such ambiguity is heightened by the fact that it may not be judicious for the stigmatized individual to disclose to many of the individuals he or she encounters.
These challenges have been documented in research with participants with
- epilepsy (e.g., Kleck, 1968),
- HIV (e.g., Chesney & Smith, 1999; Parsons, VanOra, Missildine, Purcell, & Gómez, 2004; Simoni et al., 1995),
- mental illnesses (e.g., Farina, Gliha, Boudreau, Allen, & Sherman, 1971; Quinn, Kahng, & Crocker, 2004), or
- a nonheterosexual sexual orientation (e.g., Croteau, 1996; Woods & Harbeck, 1991);
- those who are illiterate (e.g., Freeman & Kassebaum, 1956),
- infertile (e.g., Miall, 1986; Schaffer & Diamond, 1993),
- deaf (e.g., Hétu, 1996; Higgins, 1980),
- unemployed (e.g., Letkemann, 2002), or
- from a working-class background (e.g., Granfield, 1991);
- and those with past experiences of abortion (e.g., Major & Gramzow, 1999) or other trauma (e.g., rape; Koss, 1985).
Individuals or organizations that discover a concealable stigma may deny the stigmatized person employment, housing, medical care, and education. The revelation of many concealable stigmas could potentially result in
- child custody loss,
- social isolation,
- loss of job,
- abandonment by parents or close others,
- and even violence
(e.g., Corrigan & Kleinlein, 2005; Herek, 1998; Herek & Berrill, 1992).
The ambiguity of social situations combined with the threat of potential discovery makes possessing a concealable stigma a difficult predicament for many individuals.
Current Approaches to Understanding the Challenges of Concealable Stigmas
Since Goffman’s (1963) landmark book on stigmas, in which he presented evidence of the challenges involved in being discreditable, much of the work on concealable stigmas, both qualitative and quantitative, has been grounded in a variety of theories. These theories include, for example,
- [1] communication privacy management theory (e.g., K. Greene et al., 2003; Petronio, 2002),
- [2] strategic perception management (e.g., Olney & Brockelman, 2003),
- [3] identity management theory (e.g., Cain, 1991; Clair, Beatty, & MacLean, 2005; Woods & Harbeck, 1991), and
- [4] cognitive theories of secrecy (e.g., Santuzzi & Ruscher, 2002; Smart & Wegner, 2000).
Much of this work is supported by basic findings in areas as disparate as
- stigma (e.g., Crocker & Major, 1989; Goffman, 1963),
- secrecy (e.g., Kelly, 2002; Kelly & McKillop, 1996),
- self-disclosure (e.g., Derlega & Berg, 1987; Jourard, 1971; Pennebaker, 1997),
- self-presentation (DePaulo, 1992), and
- self-monitoring (Snyder, 1987).
Current conceptualizations are briefly reviewed below
[1] The communication privacy management model highlights the often complicated management of information exchange subsequent to an initial disclosure of sensitive information (Petronio, 2002). According to this scheme, when managing private information, individuals who possess the information must follow the dictates of a variety of boundary structures and rules that regulate the flow of private information between self and others.
In this way, individuals to whom the private information is disclosed must also negotiate the stigmatizing information of the other person, determining how and with whom to share that information. This heuristic model has been notably applied to the difficulties that individuals face in managing the concealment and disclosure of an HIV diagnosis. This model is useful for examining the negotiation of private information in interpersonal interactions. However, it does not address the psychological experience of this negotiation.
[2] Strategic perception management theory (e.g., Olney & Brockelman, 2003) more closely considers the psychological experience of possessing a concealable stigma. This theory focuses on the necessity for individuals with a concealable stigma to develop strategies to control their interactions with others whom they perceive to be non-stigmatized.
The theory suggests that individuals with a concealable stigma must focus closely on social interactions in order to look for clues that their interaction partner may suspect the stigma while taking an active role in guiding the nature of the interaction in such a way that the stigma can remain hidden. Rather than suggesting that individuals with a concealable stigma passively participate in social interaction, strategic perception management theory highlights the active stance that these individuals must take in negotiating others’ detection of their stigmatized status. Although it highlights the behavioral strategies that individuals with a hidden stigma use to keep their stigma hidden, this theory does not provide a framework for considering the overall psychological process that maintains this behavior.
[3] Another theory that addresses the experience of possessing a concealable stigma is identity management theory. Similar to the two theories mentioned above, it considers the management of information regarding one’s stigma. This model, though, looks specifically at the way individuals manage such information in the context of an overall identity. This theory has been most effectively applied to understanding the process of information management in the context of developing a nonheterosexual identity.
For example, Cain (1991) used this approach to highlight the difficulties that gay men face in forming a positive identity despite hiding a core part of it. This theory can also explicate the factors impacting one’s decision to reveal or hide a concealable stigma in specific environments such as the workplace. One such use of this theory considers both
- individual difference factors (e.g., self-monitoring, propensity toward risk taking) and
- contextual factors (e.g., legal protections, professional norms)
that lead one to make a decision to reveal or hide a stigmatized status (Clair et al., 2005).
Identity management theory addresses the way in which possessing a potentially concealable stigma poses challenges that must be negotiated across situations. Yet, this model does not specify the intrapersonal process by which this negotiation occurs.
[4] One model, though, does address the intrapersonal process faced by individuals who conceal a stigma. Smart and Wegner (1999, 2000) applied the cognitive preoccupation model of secrecy (e.g., Lane & Wegner, 1995) to the cognitive consequences of concealing a stigma.
Attempting to hide a stigma, like hiding any secret, leads an individual to become preoccupied with thoughts of that stigma, which has the ability to impact the individual’s well-being and social functioning. This occurs through four interrelated sequences:
- (a) secrecy causes thoughts to be suppressed,
- (b) this suppression causes intrusions of the thought,
- (c) intrusion leads to increased efforts to suppress the thought, and
- (d) the cycle of intrusion–suppression continues as long as the information is kept secret.
Data exist regarding this process as it applies to keeping secrets, generally (e.g., Lane & Wegner, 1995), and concealing an eating disorder, specifically (Smart & Wegner, 1999). The model is useful for understanding the cognitive consequences of concealing a stigma, although it does not address the cyclical nature of distress that arises from other psychological domains that may or may not be influenced by cognitive processes.
A Comprehensive Process Model
The above models address discrete aspects of possessing a concealable stigma (e.g., the process of stigma disclosure, the cognitive consequences of hiding a stigma). Yet, no existing framework or model highlights the overall psychological impact that concealing a stigma can have for an individual. Therefore, researchers who study concealable stigmas lack a cohesive model for integrating their findings. This article attempts to offer a tentative model that can guide interpretation of the literature and point to directions for future research.
The present model joins other social cognitive process models in explaining the way that person and environmental variables interact to shape eventual behavioral outcomes
- (e.g., Andersen & Chen, 2002; Downey & Feldman, 1996; Dweck & Leggett, 1988; Goldfried, 1995; Magnusson, 1990; Mischel & Shoda, 1995).
Although it is important to recognize the sway of long-standing individual traits (e.g., information-processing strategies, temperament, and biological variables) on person–situation outcomes, this model attempts to predict the cycle that anyone who conceals a stigma may encounter regardless of his or her unique predispositions.
This heuristic model rests on the premise that concealing a stigma influences the features of situations to which individuals are most likely to be attuned as well as the cognitive and affective mediators of behavior in stigma-relevant situations. In the proposed cycle, the influence of concealing a stigma extends beyond the influence of global personality traits.
The model in Figure 1 [here below] depicts the details of the process experienced by those with a concealable stigma in a stigma-relevant situation.
Figure 1. A process model of the psychological implications of concealing a stigma. CSI-Outcomes Model. Concealable stigmatized identity construction and psychological, physical, and behavioral outcomes.
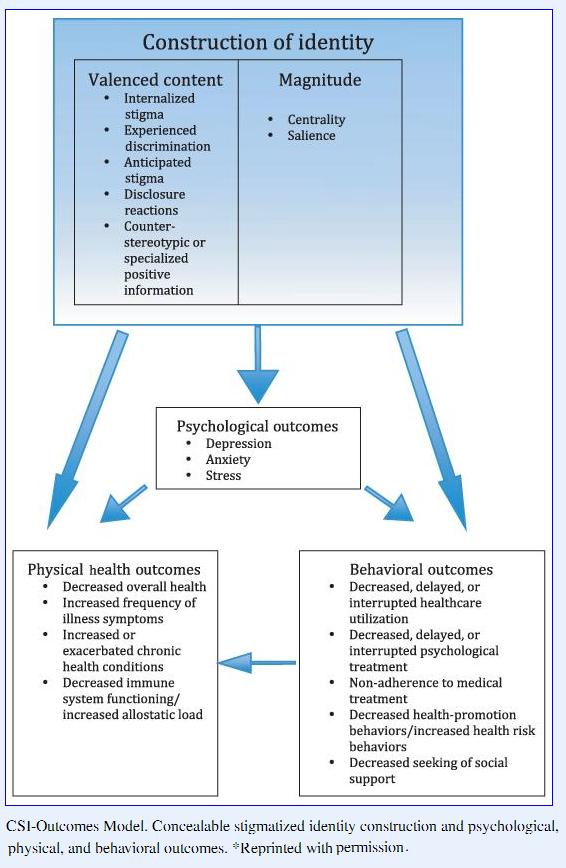
This model proposes that features of situations activate a set of internal reactions, both cognitive and affective, for individuals with a concealable stigma. These cognitive and affective responses, such as preoccupation, vigilance, guilt, and shame, are closely linked, and their influences are bidirectional. Negative cognitive patterns, such as misattribution of the source of one’s difficulties, can lead to problematic affective states, such as
- anxiety and depression (e.g., Beck, 1976; Schachter & Singer, 1962), and
- negative affective states can lead to problematic cognitive processing (e.g., Bower, 1981; Teasdale & Russell, 1983).
Both cognition and affect play a dynamic role in influencing eventual behavior and can impact behavior either separately or together.
For example,
- preoccupation with one’s undisclosed HIV-positive status may lead to anxiety in potential romantic encounters.
- Preoccupation and anxiety, alone or together, may lead to social awkwardness in these encounters.
- This behavior, in turn, affects the individual’s interpersonal environment.
The present model additionally recognizes the importance of self-evaluation in influencing the way individuals interact with their surroundings. Self-evaluation is an essential component of the present model, as individuals’ cognition, affect, and behavior influence their self-concept and perceived efficacy in any given situation.
Conversely, individuals’ self-concept and perceived efficacy influence their cognition, affect, and behavior. Thus, if one doubts his or her abilities to succeed in a given situation, this is likely to affect his or her thoughts, feelings, and actions. Within the context of the preceding example, as HIV-positive individuals think, feel, or act poorly in romantic encounters, they see themselves in a negative light in that situation in addition to viewing their ability to improve their romantic situation as limited (e.g., Burns, 1979; Epstein & Erskine, 1983; Magnusson, 1990; Markus & Wurf, 1987). Such negative self-evaluation likely will lead to problematic thoughts, feelings, and behavior in future romantic encounters.
It should be emphasized from the start that concealable stigmas vary in their level of concealability as well as in the severity and duration of their consequences. For example, infertility, which can be hidden for a long period of time, is arguably more concealable than epilepsy, which is marked by periodic seizures. Yet even infertility may not be completely concealable. For instance, relatives and friends may continually ask a couple when they plan to have children. After repeated inquiry, the infertile individual or couple must become increasingly creative to stave off suspicion of the secret stigma.
Further, a progressive illness like Parkinson’s disease results in gradual deterioration of physical abilities to the point at which symptoms become very difficult to conceal. Such gradual deterioration requires the stigmatized individuals to revise or refine their strategy for managing the stigma.
In addition, even visible stigmas, such as race or obesity, can be concealed in some types of interactions, such as those that involve telephone or Internet communication. The ease with which an individual can conceal his or her stigma no doubt influences the implications of possessing such a stigma. This article is primarily concerned with the implications of possessing a stigma that can be easily concealed. However, there is no clear boundary on the concealability continuum at which this discussion stops.
The model that follows incorporates relevant evidence from broader theories of
- stigma,
- secrecy,
- self-disclosure,
- self-presentation, and
- self-monitoring.
The description begins with the situational features that may trigger the negative psychological outcomes of concealing and then highlights the cognitive, affective, behavioral, and self-evaluative responses that occur.
The narrative explains how the cognitive, affective, behavioral, and self-evaluative consequences are interrelated and how each plays a role in perpetuating problematic psychological outcomes in a cyclical manner.
It ends with a discussion of potential ways in which this cycle may be broken as well as potential routes to investigations of the cycle. As will be seen, most of the psychological implications of possessing a concealable stigma are related to the challenges of concealing, per se, and the present review focuses closely on those challenges. Yet, simply possessing a stigma that can be concealed may be fraught with unique challenges not necessarily related to the process of concealing. This article briefly considers those challenges as well.
Situational Dependency
To understand the psychological consequences of concealing a stigma, one must understand the potential situational triggers of these consequences. Thus, the discussion of the present model begins at the level of situational influences. Here, situational influences encompass those aspects of situations that are likely to give rise to certain cognitive, affective, and behavioral outcomes (see Figure 1).
Situational factors influence cognition, affect, and behavior
- (e.g., Endler, Hunt, & Rosenstein, 1962; Epstein, 1979; Goldfried, 1995; Ross & Nisbett, 1991; Shoda, Mischel, & Wright, 1989; Spielberger, 1972).
Situational factors also influence the development of self-esteem. The self-esteem of visibly stigmatized individuals, such as women and African Americans, emerges from the meanings that individuals give to specific situations involving those stigmas (e.g., Crocker & Quinn, 2000).
Certain situations, like being the only African American student in a university lecture class, make one’s stigma particularly salient
- (Mendoza-Denton, Downey, Purdie, Davis, & Pietrzak, 2002; Steele, Spencer, & Aronson, 2002).
Relevant to the model presented here are features of situations that have differential consequences for those with a concealable stigma versus those without such a stigma. The present model proposes that certain aspects of situations directly influence the cognitive–affective mediators of behavioral outcomes in those situations (see Figure 1).
Outlined below are characteristics of situations that may bring about negative consequences for those with a concealable stigma.
Prior theorizing and work suggests that individuals with a concealable stigma experience difficulty in those situations in which
- (a) one’s stigma is made salient,
- (b) one’s concealed stigma is likely to be discovered, and
- (c) the consequences of being discovered are costly.
Stigma salience may be a concern for individuals with either visible or concealable stigmas, whereas the threat and consequences of being discovered are stressors unique to those with concealable stigmas whose stigmatized status is not fully known in all face-to-face social situations that they encounter.
[a] Salience of Stigma
Stigma salience refers to the relative accessibility of stigma-related thoughts or concerns. The salience of one’s concealable stigma in a particular situation determines the psychological experience of that situation. A stigma is salient when it is shared by many or shared by none in a given situation.
For instance, the stigma of being gay is salient at a gay pride parade attended by many other openly gay people or at a family reunion attended by no other openly gay person. Situations in which an individual perceives himself or herself to be alone in possessing the stigma may be more likely to lead to negative psychological consequences than those situations in which similar others are present. In one study, the presence of other people who shared the stigma of being gay, bulimic, or poor yielded more positive self-esteem and mood (Frable, Platt, & Hoey, 1998).
In addition to the presence or absence of similar others, the presence of stigma-related cues can make one’s concealable stigma salient.
For instance,
- baby showers can make one’s infertility salient, and research shows that infertile women find such situations to be quite difficult (e.g., Miall, 1986; Schaffer & Diamond, 1993; Whiteford & Gonzalez, 1995).
- Child-related cues could also lead to negative psychological consequences for women who have had an abortion.
- Similarly, eating-related cues can trigger negative psychological consequences for young women with bulimia (Smart & Wegner, 1999).
- Sexuality-related cues can have a similar impact for nonheterosexual individuals. In fact, a group of lesbian physical education teachers noted discomfort when supervising the girls’ locker room (Woods & Harbeck, 1991).
Again, stigma-related cues make one’s concealable stigma salient and trigger negative psychological consequences as a result.
[b] Threat of Discovery
In addition to stigma salience, the threat of discovery in a given situation may negatively impact individuals with a concealable stigma. Threat of discovery is high in situations that challenge or question one’s status or identity.
Endler and Bain (1966) found that status-related situations, such as job interviews, made working-class students more anxious than did non-status-related situations, such as taking a final exam or giving a speech, possibly because working-class students feared detection of their hidden background in those situations related to socioeconomic status.
Also relevant is the finding by Lee and Craft (2002) that all of the participants in a genital herpes support group reported avoiding sex-relevant relationships to some degree following their diagnosis.
Situations in which one may be forced to answer questions related to a stigmatized status raise the threat of discovery. In such situations, individuals with a hidden stigma face the choice between telling the truth and facing the ensuing interpersonal consequences or deceiving and facing the mostly intrapersonal consequences. Situations in which one is asked pointed questions about a hidden status make hiding difficult and distressing. Being asked about HIV status by a presumably HIV-negative potential sex partner will probably lead to stigma-related distress for a person with HIV.
[c] Consequences of Being Discovered
The perceived consequences of being discovered in a given situation can also distress individuals with a concealable stigma.
The revelation of many concealable stigmas, such as
- homosexuality,
- HIV infection, or
- mental illness
may cause
- rejection,
- social isolation,
- abuse,
- employment and housing discrimination,
- disownment by parents or close others, and even
- violence
(e.g., Corrigan & Kleinlein, 2005; Herek, 1998; Herek & Berrill, 1992).
In 2003 alone, close to 1,500 lesbian, gay, or bisexual individuals reported being victims of hate crimes in the United States (Federal Bureau of Investigation, 2004). Nearly half of those bias-related incidents involved simple or aggravated assault. Religious minorities reported a comparable incidence of bias-related victimization. Data are unavailable regarding the settings in which this victimization occurred. Yet, an individual who knows that such consequences could occur if someone discovered his or her stigma would likely avoid such situations or endure them uneasily.
Of course, these reported figures of victimization-related incidents may be substantially lower than the actual occurrence of such crimes because of the victims’ fear of further harassment or rejection upon disclosing the crimes to authorities.
In a recent survey, most community-based HIV/AIDS service organizations presented numerous instances of their clients losing or being demoted in their jobs and losing housing and child visitation upon disclosing their HIV-positive status (Lange, 2003).
Additionally, research suggests that stigma-related victimization may lead to more negative psychological consequences than non-stigma-related victimization (Herek, Gillis, & Cogan, 1999).
Thus, when entering situations in which discovery can lead to negative consequences, individuals with a concealable stigma may encounter substantial psychological difficulties.
Cognitive Implications
This section highlights the cognitive consequences unique to concealing a stigma. In the proposed model, challenging situations (discussed previously) as well as affective and self-evaluative challenges (discussed later) lead to these cognitive difficulties. The relationships between cognition and affect as well as between cognition and self-evaluation are bidirectional, meaning that cognitive difficulties can also lead to affective and self-evaluative distress. The link between situation and cognition is unidirectional from situation to cognition.
Thus, cognition impacts situations only through its impact on behavior and self-evaluation (see Figure 1). Experimental data from other areas of psychology support the location and functioning of cognition in the overall model in the manner described here
- (e.g., Bandura, 1988; Bower, 1981; Bowers, 1973; Meichenbaum, 1972; Teasdale & Russell, 1983).
Preoccupation
As noted earlier, stigma salience may trigger negative psychological consequences for individuals with a concealable stigma. Salience of the secret can be helpful, though, as it reminds the secret keeper to avoid disclosing topics related to his or her secret.
However, even though it serves such a protective function, keeping the secret in constant awareness can also be distressing, as it makes the secret more available and thus more likely to be leaked (Lane & Wegner, 1995).
The notion that thought suppression leads to thought intrusions has been supported by research showing that participants who are instructed to stop thinking about an object cannot easily do so and that thoughts of this object emerge when efforts at suppression cease — the so-called rebound effect (Wegner, Schneider, Carter, & White, 1987).
Further, instructions of thought suppression seem to make the suppressed thought more likely to intrude upon consciousness, especially under conditions of additional cognitive tasks (Wegner & Erber, 1992; Wegner, Erber, & Zanakos, 1993). It is not surprising that such intrusions may lead the secret keeper to fear that he or she will reveal the secret and, thus, to increase suppression efforts. A series of studies by Lane and Wegner (1995) elucidate the mechanisms of the cognitive model of secrecy. These studies suggest that secrecy leads to intrusive thoughts by increasing attempts at thought suppression.
These findings are applicable to the experience of concealing a stigma.
Smart and Wegner (2000) noted that concealing a stigmatized status can lead to unique hidden costs not shared by individuals with a visible stigma. The cognitive preoccupations of concealing one’s stigma can be tremendous and hence have been labeled as a private hell (Smart & Wegner, 2000).
For example, Smart and Wegner (1999) demonstrated the cognitive hold that stigma can have on women with an eating disorder. The researchers assigned women with and without an eating disorder to participate in an interview in which they were asked to role play someone with or without an eating disorder status. The interviewer asked questions designed to make one’s eating disorder salient, for example, “Does anyone ever tell you that you have strange eating habits?” Participants were then asked to complete self-report measures of their thought processes during the interview. In a subsequent study, participants responded to a Stroop task including words related to eating disorders.
The results of these studies revealed that women with an eating disorder who were instructed to conceal their stigma were more likely to report thought suppression and thought intrusions during the interview than were women in the other conditions, even those who had an eating disorder and were instructed to reveal it. The results of the Stroop task further supported these findings. That is, the women with an eating disorder who hid their disorder demonstrated slower response time to the eating disorder-related words, suggesting interference in cognitive processing of this information.
Thought intrusions may lead to fixed thinking in which the secret consumes the individual’s daily life and leads to more disordered thinking (Wegner & Lane, 1995). The inhibition of the expression of emotion-laden topics may be associated with rumination about those topics, supporting the existence of the rebound effect described above (King, Emmons, & Woodley, 1992). However, the rebound effect may be limited to thoughts about personally irrelevant objects and may not occur for more personal, difficult, or emotional thoughts (Kelly & Kahn, 1994; Roemer & Borkovec, 1993; Wegner & Gold, 1995).
It has been suggested that individuals may protect themselves from such personal thoughts by engaging in special defense strategies, such as distraction, against these thoughts (Kelly & Kahn, 1994). Some people may have quite emotional or difficult thoughts about their stigma, especially if they view it as sick, sinful, or deviant. Whether the rebound effect occurs for individuals who suppress such thoughts about a concealable stigma remains to be seen.
Increased Vigilance of Stigma Discovery
Confronting a threatening stigma-related situation (see situation in Figure 1), being under ample affective distress (see affective implications in Figure 1), and perceiving oneself as incapable of hiding a stigma (see self-evaluative implications in Figure 1) could lead to increased vigilance for cues that one’s stigmatized status may be suspected (see the links from situation, affective implications, and self-evaluative implications to cognitive implications in Figure 1).
Individuals with a concealable status may protect themselves by closely attending to social interactions, monitoring the actions and discerning the potential perspectives of interaction partners. This may be a useful strategy for determining whether an interaction partner suspects a stigma and how this person may react (or be reacting) to knowledge of this stigma. This also allows the stigmatized person to think ahead to potential paths that can be taken if the interaction partner, in fact, ascertains the hidden stigma. Being so vigilant in social interactions, though, can have negative psychological consequences. The link in the present model between the cognitive and behavioral implications suggests that such vigilance may negatively impact the interpersonal behavior of an individual with a concealable stigma.
Frable, Blackstone, and Scherbaum (1990) found evidence of this in their study of mindfulness in women with master status conditions, which were defined as those traits that occur relatively infrequently in the U.S. population, whether valued or devalued (e.g., attractiveness, deformity), visible or concealable (e.g., wealth, poverty).
In their study, mindfulness involved paying close attention to one’s surroundings and thinking ahead to potential paths that social situations may take. They cited evidence that supports the construct of mindfulness as the ability to adjust to ever-changing situations (e.g., Chanowitz & Langer, 1981; Langer, 1989; Langer & Piper, 1987).
The master status conditions were analyzed in four groups:
- (a) visibly devalued (i.e., being facially scarred, 60 pounds overweight, or Black),
- (b) invisibly devalued (i.e., having a bisexual identity, rape history, or incest history),
- (c) visibly valued (i.e., being physically attractive, having been defined as being either a prom queen or model), and
- (d) invisibly valued (i.e., being very wealthy, athletic, intelligent, or talented).
The researchers paired each master status individual with a non-master-status individual in order to determine whether master status individuals were more mindful in social interactions. They found that, despite the fact that those people with any master status conditions exhibited more mindfulness in social interactions, those with a concealable status were more likely to take the perspective of their interaction partner and remember what their partner said than were individuals with a visible master status.
Suspiciousness
Concealing a stigma in difficult situations may make the stigmatized person suspicious.
In one study, women who role played having a lesbian identity and concealing this identity engaged in more paranoid social cognition in the interaction than did women who disclosed this pretend identity or those who were assigned to a neutral role play (Santuzzi & Ruscher, 2002). Their thoughts were marked by self-consciousness and expectations of negative evaluation from their interaction partner. As this effect was strong enough to be found in a study that asked individuals to role play possessing a concealable stigma, it seems that this suspiciousness would be even greater for those who actually possess the stigma.
Similar to participants in the study by Frable et al. (1990), participants in this study may have been suspicious that their interaction partner was detecting indications of the stigma. Despite the limitations of this study (e.g., the participants were only role playing having a concealable stigma, not actually stigmatized), the notion that individuals with a concealable stigma may be paranoid is consistent with the overall association between secrecy and cognitive difficulties.
Individuals with a visible stigma escape many of the cognitive burdens faced by individuals with a concealable stigma. Undoubtedly, individuals with either a visible or concealable stigma may experience cognitive difficulties such as preoccupation, vigilance, and suspiciousness (e.g., Mendoza-Denton et al., 2002). Yet, the cognitive difficulties of concealing a stigma are of a unique nature in that they are additionally characterized by
- cognitive preoccupation with giving off clues of the stigma,
- vigilance of the possibility that the stigma is suspected, and
- suspiciousness that one’s stigma has been discovered.
For an individual with a concealable stigma, these challenges pave the way for
- negative affective states,
- behavioral difficulties, and
- negative self-evaluation
in accordance with the present model, as addressed in the following sections.
Affective Implications
As noted previously, the present model draws on past experimental evidence to conceptualize the influence of cognition and affect as bidirectional, with each influencing the other in addition to influencing behavior and self-evaluation (e.g., Bower, 1981; Bowers, 1973; Meichenbaum, 1972; Teasdale & Russell, 1983).
Further, situational features impact both cognition and affect (e.g., Mischel & Shoda, 1995). The cognitive preoccupation, avoidance, and suspiciousness experienced by individuals with a concealable stigma are proposed to foster negative affective states, which are reviewed below. These negative affective states, in turn, may increase preoccupation, vigilance, and suspiciousness.
The emerging area of secrecy research (e.g., Kelly, 2002) provides evidence that possessing a secret, such as a concealable stigma, may lead to emotional strain. Keeping one’s stigma hidden is likely to be motivated by fears of negative evaluation and the avoidance of rejection in situations of the type described earlier.
Although keeping shameful secrets permits individuals to escape potential evaluation and rejection, Kelly (1998) reviewed substantial evidence suggesting that those who keep personal secrets tend to be more lonely, shy, introverted, and socially anxious and have a higher need to be alone than do those without a tendency toward secret keeping
- (e.g., Cepeda-Benito & Short, 1998; Cramer & Lake, 1998; Gesell, 1999; Ichiyama, Colbert, Laramore, & Heim, 1993; Larson & Chastain, 1990).
Secret keeping, by nature, is shameful. The mere act of hiding information about a stigma may lead an individual to believe that the stigma-related information is shameful simply because it is worthy of being hidden (Derlega, Metts, Petronio, & Margulis, 1993; Kelly, 2002).
Research attests to the notion that secrecy is linked to problematic self-perceptions (see Kelly, 2002, for a thorough review of this research). For example, individuals who concealed an ambiguous test score rated the score more negatively than individuals who disclosed the very same test score (Fishbein & Laird, 1979). This particular study suggests that those who concealed the test score came to see this information more negatively than those who did not simply because they engaged in the processes associated with hiding.
Individuals who conceal information about themselves over a substantial period of time may come to perceive this concealed information as shameful and see their overall selves in a negative light. The self-perception model of secrecy is derived from Bem’s (1972) theory that people use their behavior to label ambiguous internal states (Fishbein & Laird, 1979; Kelly, 2002).
Some research has specifically addressed the relationship between stigma-related secrets and negative emotions.
Using an 11-day experience sampling methodology, Frable et al. (1998) found that students at an elite university who possessed a concealable stigma reported
- lower social confidence,
- higher anxiety,
- higher depression, and
- lower self-esteem
than did visibly stigmatized and nonstigmatized students.
In their concealable and stigmatized group, the researchers included those students who indicated that they were gay, lesbian, or bisexual; bulimic; or from low-income families. They found that participants with a concealable stigma reported more negative affect than did other participants.
Frable et al. (1998) provided data demonstrating that the greater social isolation of individuals with a concealable stigma does not explain these findings. However, they did find that the presence of similar others increased the positive affect of these participants.
Sadly, though, these participants were the least likely to experience such contact. The fact that participants with a concealable stigma experienced more negative affect than even those participants with a visible stigma suggests that a stigma’s concealability moderates the link between possessing a stigma and experiencing negative emotion.
The cognitive difficulties of concealing can lead to emotional difficulties.
One test of this link followed 442 women for 2 years after having had an abortion (Major & Gramzow, 1999). Women who perceived abortion as stigmatizing reported a greater need to keep their abortion a secret from close others. This secrecy was associated with more thought suppression and intrusions of the type described by Lane and Wegner (1995) in their preoccupation model of secrecy. Increased thought suppression and intrusions were associated with increased psychological distress (i.e., depression, anxiety, and hostility) over the 2-year follow-up.
Disclosure of feelings related to the abortion moderated the relationship between thought intrusions and distress. That is, disclosure was associated with decreases in anxiety, depression, and hostility among women who reported experiencing intrusive thoughts of their abortion, but it was unrelated to these variables among women who did not report intrusive thoughts. This study supports the link from cognition to affect in the present model (see Figure 1).
Other studies provide evidence that concealing a nonheterosexual orientation is associated with more emotional distress, such as depression, than is disclosing this orientation.
In one such study, gay men who concealed reported more depression and poorer overall psychological well-being than did those who disclosed (Ullrich, Lutgendorf, & Stapleton, 2003). In a 14-day experience sampling study, 33 lesbians and 51 gay men reported greater psychological well-being (e.g., self-acceptance, purpose in life, autonomy, mastery) on days when they disclosed their sexual orientation compared with days when they concealed their orientation (Beals, 2004). The individuals’ experience of social support mediated this association. Also, active suppression of thoughts about sexual orientation predicted lower psychological well-being at the end of each day and at 2-month follow-up.
Those who hide a history of mental health treatment may similarly experience emotional distress. Both avoidance of stigma-related disclosure as well as avoidance of individuals who might discover one’s mental health history were associated with greater rates of
- helplessness,
- hopelessness,
- sadness, and
- confused thinking
in 164 psychiatric patients (Link, Mirotznik, & Cullen, 1991).
Secrecy partially explained the correlation between the perceived mental illness-related discrimination and negative affect. Hiding a stigma prevents individuals from engaging in corrective experiences in which they learn that others may not be as likely as initially supposed to discriminate against them because of their status. This may be one way in which concealing leads to distress. This possibility is further explored in following sections (see the Behavioral Implications and Self-Evaluative Implications sections).
Concealing an HIV status may be associated with unique consequences not associated with concealing other stigmas. In fact, more research exists on the affective consequences associated with the stigma of HIV infection than on any other concealable stigma.
Diseases that are progressive and incurable, that are not well understood by the public, and for which the person with the disease can be seen as morally responsible for contracting lead to difficult psychological consequences (Goffman, 1963; Herek, 1999; Jones et al., 1984).
Because HIV combines these features in addition to myriad personal, legal, and social implications, people with HIV are particularly vulnerable to emotional distress in relevant situations. People with HIV who disclose their status may experience emotional distress as a result of the ensuing rejection, abuse, or violence (North & Rothenberg, 1993; Parsons et al., 2004). However, those who conceal an HIV-positive status may also experience emotional distress.
In one study of ethnically diverse HIV-positive men and women, those who had not disclosed their HIV status to their sex partners exhibited more emotional distress than did those who had disclosed this information (Kalichman & Nachimson, 1999). Specifically, participants who had not disclosed their HIV status indicated more
- psychoticism,
- somatic anxiety,
- hostility, and
- phobic anxiety
on a mental health symptom inventory.
In another study at an HIV clinic in France, 174 HIV-positive patients reported that fear of rejection was the main reason for not revealing their HIV status (Lévy et al., 1999). Nearly one quarter of this sample waited at least 1 year before disclosing their HIV status to another person. Three quarters of participants who disclosed their HIV status asked that their secret be respected. Still, 30% of these individuals later learned that their confidence had been broken, and another 18% suspected that it had been broken. It is interesting that only half of the participants planned their disclosure. The other half reported that their disclosure was a spontaneous act in response to the increasingly unbearable psychological distress of suppressing key information about their identity (i.e., the link from affect to disclosure in Figure 1).
The findings by Lévy et al. (1999) challenge the widely held assumption that HIV disclosure occurs as a result of social responsibility or special trust in another person. These findings also speak to the emotionally distressing nature of concealing a stigma.
Still, these findings challenge the notion that disclosure of a concealable stigma always results in positive emotional consequences. In fact, the authors noted that many of their participants reported anxiety, uneasiness, and sadness after disclosing their HIV status.
Clearly, individuals with HIV face unique consequences not faced by those with a stigma that is visible to others.
Family members of an individual with HIV may experience similar emotional repercussions as a result of concealing a courtesy stigma — the stigma of being associated with a stigmatized individual (Goffman, 1963). Preliminary evidence for the emotional consequences of bearing a courtesy stigma shows that children who keep their mothers’ HIV-positive status a secret are likely to experience some degree of anxiety, mostly related to concerns of their secret being found out and a desire to protect their mothers (Murphy, Roberts, & Hoffman, 2002).
Ethnicity may influence the association between HIV concealment and emotional distress. For Latina women with HIV, greater emotional distress was associated with greater disclosure, whereas such a relationship was not found for African American or Caucasian women (Comer, Henker, Kemeny, & Wyatt, 2000). This difference may be due to cultural differences in reactions to this particular stigma or cultural differences in the personal experience of this stigma.
Future researchers will need to determine the causal direction between disclosure and emotional distress. Yet, these studies offer evidence that disclosing a stigma, especially one that is very likely to elicit negative reactions from others, is not always associated with positive psychological outcomes.
It seems that when shame or fear of rejection motivate secrecy in given situations, individuals with a concealable stigma may be particularly likely to suffer emotionally. Two of the above studies bring together research on the cognitive as well as affective implications of concealing a stigma and offer support for the cognitive–affective causal link in the current model (see Figure 1).
Specifically, Major and Gramzow (1999) and Beals (2004) offered evidence that active suppression of stigma-related information leads to greater psychological distress, likely as a consequence of stigma-related thought intrusions. These studies suggest that, in certain situations, concealing may lead to cognitive burdens that lead to emotional difficulties. Whereas individuals with a visible stigma face the emotional stress of being devalued, individuals with a concealable stigma must choose between this stress and the emotional stress of hiding.
Behavioral Implications
Possessing a visible stigma may cause disruptions of interpersonal interactions (e.g., Hebl, Tickle, & Heatherton, 2000). Concealing a stigma may also cause disruptions in interpersonal interactions, albeit through different mechanisms than with visible stigmas. Specifically, concealable stigmas may lead to
- interpersonal disruptions through increased self-monitoring and impression management,
- behavioral performance deficits,
- increased social avoidance and isolation, and
- the increased importance of feedback in shaping behavior.
These behavioral implications are reviewed below. As suggested in the present model, cognitive and affective states mediate the influence of situational features on this eventual behavior (e.g., Mischel & Shoda, 1995). Also, as is reviewed later, behavior and self-evaluation influence each other, and behavior also influences the nature of subsequent situations.
Impression Management and Self-Monitoring
Individuals with a concealable stigma must decide whether and how to present their stigma according to their assessment of a given situation. Clearly, those with a visible stigma cannot choose whether to present their stigma; they can only decide how to manage the impression it makes in various situations.
Whereas visibly stigmatized individuals may engage in impression management strategies to compensate for a perceived lack of normality or competence, individuals with a concealable status engage in them to prevent their stigma from being discovered. Individuals with concealable stigmas may expend much energy to ensure that stigma-related “leakages” do not occur (Goffman, 1963).
However, the avoidance of these information leakages cannot be guaranteed, and individuals must use additional energy to repair their self-presentations when they unintentionally reveal stigma-related information. An individual who is hiding a Parkinson’s disease diagnosis would have to quickly concoct an explanation for his uncontrollably trembling hands. Creating an excuse, such as nervousness, may be complicated, as convincing explanations are not always easy to create. Clearly, conveying a nonstigmatized status requires much conscious effort on the part of the stigmatized individual, and even then it is not guaranteed to work without fail.
Ample research on impression management and deception attests to the distress associated with concealing information — such as a romantic affair — and presenting a false impression of oneself— such as lying about one’s sexual orientation
- (e.g., Burgoon & Buller, 1994; DePaulo, Ansfield, Kirkendol, & Boden, 2004; Vohs, Baumeister, & Ciarocco, 2005).
Evidence suggests that many people with a concealed stigma engage in impression management behaviors. Individuals reporting this behavior include
- lesbians and gay men (Cain, 1991; Pachankis & Goldfried, 2006; Woods & Harbeck, 1991),
- former psychiatric patients (Herman, 1993; Link et al., 1991; Matthews & Harrington, 2000),
- those who are involuntarily childless (Miall, 1986), and
- those with invisible physical disabilities (Matthews & Harrington, 2000; Rintamaki & Brashers, 2005).
Three quarters of the gay male students in a study by Pachankis and Goldfried (2006) reported that they had attempted to change their behavior as a result of fear of being rejected because of their sexual orientation.
Participants noted such attempts as
- modifying the tone or content of their speech,
- modifying their mannerisms (e.g., posture, gestures),
- changing the way they walked,
- lying (mostly about the sex of a romantic partner), and
- trying to appear more masculine (or less feminine).
Such behaviors can be conceptualized as attempts to avoid making the concealable stigma obvious and thus to avoid the ensuing rejection and negative evaluation. Figure 1 depicts this relationship between affective implications (e.g., fear of negative evaluation) and behavioral implications (e.g., avoidance).
Impression management attempts are associated with noticeable consequences, including verbal and nonverbal behaviors such as increased response latency and decreased eye contact (J. O. Greene, O’Hair, Cody, & Yen, 1985).
Deceivers display a variety of noticeable verbal and nonverbal behaviors including speaking in a higher pitched voice and displaying more hesitation, eye blinking, and speech errors than do those who are telling the truth (see DePaulo, 1992, for a review). DePaulo (1992) explained such findings in terms of the increased anxiety experienced by those who are motivated to deceive. It remains to be seen whether such consequences exist for those who are motivated to conceal a stigma, specifically.
The construct of self-monitoring is closely tied to impression management (e.g., Snyder, 1987). People may attempt to change their behavior out of fear of being identified by their stigma. Lesbian, gay, and bisexual adolescents may engage in continual self-monitoring of their behavior lest they give off clues of their discreditable sexual orientation (Hetrick & Martin, 1987).
Although past research has not addressed the link between concealment of a stigma and increased self-monitoring behavior, this link may exist, given the evidence of increased fear of negative evaluation and the potentially strong motivation to appear nonstigmatized for individuals who conceal a hidden devalued trait.
Social Avoidance and Isolation
Individuals with a concealable stigma may also choose to completely avoid situations in which they may be rejected. In fact, research suggests that avoidance of others is a common strategy for circumventing the negative cognitive and affective consequences of concealing a stigma
- (e.g., Corrigan & Matthews, 2003; Croteau, 1996; Link et al., 1991; Remennick, 2000).
Goffman (1963) noted that individuals with a concealable stigma cope with their stigma by avoiding close relationships. Fears of rejection and negative evaluation may prevent an individual from disclosing and may also prevent him or her from attaining necessary support.
Many researchers have documented the importance of support in the lives of stigmatized individuals
- (e.g., Goldfried & Goldfried, 2001; Hershberger & D’Augelli, 1995; Peterson, Folkman, & Bakeman, 1996).
Possessing a stigma that is invisible to others leaves individuals with the choice to remain quiet about their stigma and, thus, to miss out on opportunities to receive important social support.
Many individuals with a concealable stigma may, in fact, live without such support. Individuals who are gay, bulimic, or poor may be less likely to be in social situations than are their visibly stigmatized or nonstigmatized peers (Frable, Platt, & Hoey, 1998).
Lesbian, gay, and bisexual adolescents are quite adept at hiding their stigma, which can lead them to experience increased isolation and distress (Hetrick & Martin, 1987). These youth seem to experience more social anxiety than do their heterosexual peers, which may be related to less contact with supportive friends or adults who could serve as a buffer against stigma-related distress (Safren & Pantalone, 2006).
The relinquishment of support may also make it hard to form a positive identity. One study found that gay men who concealed their sexual orientation had difficulty forming a positive gay identity (Frable, Wortman, & Joseph, 1997). Concealment may also preclude the receipt of even more essential help. For instance, Jones et al. (1984) reported that fear of negative evaluation may lead some mentally ill individuals to forfeit receiving mental health treatment under their health insurance coverage (see the affective–behavioral path in Figure 1).
Increased Importance of Interpersonal Feedback
Another unique behavioral consequence of possessing a hidden stigma may be the relative importance of feedback in shaping behavior. Hiding a stigma precludes feedback regarding the stigma and, thus, the formation of positive evaluations of one’s entire self — stigma and all. Therefore, the feedback that one receives upon initially disclosing a stigmatized aspect of his or her identity may greatly impact feelings of self-worth and subsequent behavior.
McKenna and Bargh (1998) examined the impact of positive and negative feedback on the behavior of individuals who disclosed their concealable stigma through an online message-posting group. For 3 weeks, the researchers compared the message postings of
- visibly stigmatized individuals (e.g., those who stuttered or were overweight or bald),
- nonvisibly stigmatized individuals (e.g., those who were gay, used drugs, or had a sexual fetish),
- and those who were not stigmatized (e.g., those who had various popular culture interests).
Participants with a concealable devalued trait posted messages less frequently in response to negative feedback and more frequently in response to positive, affirming feedback than did other participants. Whether someone reveals a strongly stigmatized identity may depend on the reactions that he or she expects to receive or has received in the past. Some individuals with a concealable stigma, for example, may have been treated as awkward, dangerous, incompetent, or insecure upon previous disclosure of their stigma. It seems reasonable, then, that the feedback that an individual receives about his or her stigmatized identity has the potential to shape subsequent behavior, including whether to disclose the stigma in the future, through the process outlined in the model depicted in Figure 1.
Maladaptive Behavior in Close Relationships
Individuals with a concealable stigma may also face unique challenges in their close relationships. Individuals with HIV, for example, note that close relationships are sources of stress (Harvey & Wenzel, 2002). Goffman (1963) suggested that when a stigma is concealable, short-term interactions may proceed quite normally. However, longer term relationships may suffer, especially when the individual with a concealable stigma engages in attempts to pass as nonstigmatized.
Much research attests to the importance of self-disclosure for the development and maintenance of close relationships (e.g., Cozby, 1972; Derlega & Berg, 1987; Halverson & Shore, 1969).
Concealment can lead to feelings of guilt or anxiety in a close relationship, and it may also prevent the concealer from accessing the benefits of becoming fully known to another person. Disclosure, though, can also lead to close relationship difficulties. For instance, if someone conceals a stigma from his or her close partner for many years, the partner is likely to react poorly when and if this information is ever disclosed. As more time passes, the concealer may feel increasingly guilty that he or she has duped a close other or increasingly anxious that his or her secret stigma may be discovered.
Summary
Concealing a stigma seems to be associated with a range of behavioral difficulties including
- self-monitoring,
- impression management,
- social avoidance and isolation,
- the increased impact of others’ feedback on future behaviors, and
- challenges to close relationships.
The model presented in Figure 1 proposes that the cognitive and affective implications of concealing a stigma cause these behavioral difficulties.
Similar to the cognitive–affective– behavioral rejection sensitivity model of Downey and Feldman (1996), in which an individual comes to anxiously expect, readily perceive, and subsequently overreact to social rejection, the present model suggests that negative mood states and cognitive biases lead to the behavioral outcomes reviewed here.
For instance, increased preoccupation (Smart & Wegner, 1999) or increased vigilance (Frable et al., 1990) may impact behavior in such a way that the stigmatized individual may appear distracted or uninterested.
In addition, the increased anxiety that accompanies deception may lead to behavioral consequences, such as increased response latency or decreased eye contact (DePaulo, 1992).
At this point, evidence supports the notion that individuals who conceal a stigma experience behavioral consequences not necessarily experienced by those with a visible stigma. Many agree that cognition and affect impact the behavior of all people
- (e.g., Bem & Allen, 1974; Bowers, 1973; Mischel & Shoda, 1995),
but more evidence is needed to support the notion that cognition and affect impact the behavior of individuals with a concealable stigma, specifically. This will help to further verify the process of the present model.
Self-Evaluative Implications
In addition to the cognitive, affective, and behavioral consequences of concealing a stigma, the self-evaluative consequences of concealing and the interaction between those consequences and the consequences discussed above must also be considered. Many have recognized the importance of considering self-evaluation in the context of cognition, affect, and behavior as in the model proposed here
- (e.g., Bandura, 1977; Burns, 1979; Epstein & Erskine, 1983; Goldfried & Robins, 1982; Magnusson, 1990; Markus & Wurf, 1987).
As described below, hiding a stigma is likely associated with unique self-evaluative implications that interact with all of the other psychological implications discussed thus far, serving to maintain the distressing cycle of concealment.
If an individual hides information related to his or her stigma, he or she may escape the direct experience of prejudice and discrimination directed toward that stigma. However, it is unlikely that an individual can escape knowledge that society devalues the stigma.
Recognizing others’ devaluation of one’s stigma may lead to negative self-regard. Although stigmatized individuals are not necessarily at risk for experiencing lower self-esteem than non-stigmatized individuals, most of the studies that support this notion have been conducted with visibly stigmatized individuals (see Crocker & Major, 1989, for a review). It is possible that concealing a stigma may lead to self-evaluative difficulties not experienced by those who benefit from the protective properties of membership in a visibly stigmatized group. This possibility is elaborated below.
Identity Ambivalence
Hiding a stigmatized core aspect of oneself may lead to identity ambivalence — an inconsistent view of oneself across situations or time. Working-class students at an elite ivy league law school have been shown to adopt identities and self-presentations consistent with the identities and behaviors of their classmates from elite social classes (Granfield, 1991). The concealment of this working-class background allowed students to participate in the elite law school culture, reaping the rewards of high paying internships and job offers. However, the costs of such concealment included feelings of guilt, fraudulence, and betrayal of the social class and families from which they came. Identity ambivalence, then, is one way that concealing a stigma may result in negative self-evaluations.
Lack of Access to Group-Based Self-Protective Attributions
Individuals with a concealable stigma cannot access the beneficial self-evaluative properties of stigma described by Crocker and Major (1989). Examples of these benefits include attributing negative feedback to one’s stigmatized group membership rather than one’s personal shortcomings or comparing oneself to others who share the stigma instead of to those who are not stigmatized.
Individuals with a concealable stigma who are not able to access these group-based protections may come to internalize the negative feedback that they receive, which may result in negative self-evaluations and low self-esteem.
Negative View of Self
Data suggest that individuals with a concealable stigma may experience lower self-esteem than do individuals with a visible stigma or no stigma at all (Frable et al., 1998). This lower self-esteem may follow either the greater attributional ambiguity experienced by those individuals who cannot attribute negative feedback to stigmatized group membership or from the diminished opportunity to compare oneself with other members of the stigmatized group (see above). In fact, participants who had a concealable stigma in the study by Frable et al. (1998) were least likely to find themselves in the presence of similar others, a fact that the authors suggest could have led to these participants’ lower self-esteem.
Low self-esteem in HIV-positive gay men has been shown to lead to the avoidance of seeking potentially beneficial social support (Nicholson & Long, 1990). In a separate study of people living with HIV, avoidance of potential social support was shown to lead to increased psychological distress (Heckman et al., 2004).
This cycle of low self-esteem, avoidance, and distress is one likely way in which concealing a stigma may lead to negative psychological outcomes, consistent with the model presented in this article.
Diminished Self-Efficacy
Self-efficacy, an individual’s belief that he or she can effectively perform a desired behavior under specified conditions, plays an important role in the present model. Experimental evidence supports the placement of self-efficacy within the domain of self-evaluation in the present model, where it impacts and is impacted by the cognitive, affective, and behavioral components of the cycle
- (e.g., Bandura, 1988; Bandura, Adams, & Beyer, 1977; Bandura, Cioffi, Taylor, & Brouillard, 1988; Bandura, Reese, & Adams, 1982; Cervone, Kopp, Schaumann, & Scott, 1994; Salovey & Birnbaum, 1989).
The findings of a study by Kalichman and Nachimson (1999) with a sample of 266 sexually active HIV positive men and women tentatively support the links between self-efficacy and behavior in the context of concealing. In this study, concealing an HIV-positive status from sex partners was associated with low self-efficacy for HIV disclosure, less condom use, and less condom-use self-efficacy. Further, individuals who concealed their HIV-positive status from their sex partners reported greater affective distress including hostility, somatic anxiety, psychoticism, and phobic anxiety than those who disclosed their status. This affective distress may be the cause and the result of low self-efficacy.
Beyond suggesting that concealing a stigma is associated with affective, behavioral, cognitive, and self-evaluation outcomes, this study offers some support for specific links in the present model (e.g., the link between self-efficacy and behavior).
Maintenance of the Overall Cycle Through Self-Evaluation
Besides experiencing the self-evaluative implications that directly arise from concealing a stigma (such as increased identity ambivalence and lack of access to group-based attributions), one may also form a negative view of oneself simply as a result of experiencing the negative cognitive, affective, and behavioral implications reviewed in the previous sections.
For example, a negative self-image can impact
- cognitions (e.g., “My secret stigma is shameful and I am a worse person for possessing it”),
- affect (e.g., depression, anxiety), and
- behavior (e.g., impression management attempts to conceal the shameful stigma, the avoidance of situations likely to heighten shame-related cognition and affect).
Each of these domains, in turn, can further heighten negative self-evaluation. Links highlighting the bidirectional influence of self-evaluation on cognition, affect, and behavior are depicted as double-headed arrows in Figure 1.
Thus, although individuals with a concealable stigma may escape the negative effects of direct discrimination, they may experience psychological complications arising from the need to hide their stigma;
- a lack of genuine feedback about themselves; and
- the consequences of problematic cognition, affect, and behavior on their self-evaluation.
Review of the Cycle
So far, this article has reviewed evidence suggesting that individuals with a concealable stigma face unique psychological consequences as a result of possessing discrediting information that must be negotiated across many situations. These psychological consequences fall under the domains of
- cognition,
- affect,
- behavior, and
- self-evaluation,
and the present model incorporates these domains in a process model.
Figure 1 illustrates the proposed links of this model and highlights the interrelated and cyclical nature of the individual domains reviewed above.
In many interpersonal situations, the individual with a concealable stigma must decide whether to conceal or disclose the stigma. Certain aspects of the situation influence one’s cognitive–affective functioning and ultimately the decision to disclose. According to the model, concealment is most difficult in those situations in which
- the stigma is salient,
- the threat of it being discovered is high, and
- the consequences of it being discovered are severe.
An individual with a concealable stigma will likely face cognitive and affective consequences, such as
- self-consciousness,
- vigilance,
- shame, and
- guilt
when concealing in these situations.
These cognitive and affective components are closely related and impact each other. Cognition and affect lead to behavioral consequences including
- impression management,
- social avoidance and isolation,
- increased importance of feedback from others, and
- impaired relationship functioning.
The experience of these difficulties may, then, lead to negative self-evaluative consequences such as identity ambivalence and low self-efficacy. For example, avoidance of social situations may lead to low self-esteem as one comes to see oneself negatively because he or she is isolated from others.
Negative self-evaluation may itself lead to cognitive, affective, and behavioral difficulties in encountered situations (e.g., an individual with low self-efficacy for concealing may avoid social interactions).
Finally, one’s past behavior and self-evaluation of that behavior influences the experience of future interpersonal situations, including the decision to disclose or conceal in those situations or to possibly avoid such situations altogether.
Consider the case of a gay male teenager who decides to conceal his sexual orientation as a function of the stigma salience, threat of discovery, and consequences of discovery at a family reunion.
- He may find himself burdened by intrusive thoughts or dread about the stigma in various encounters at this event.
- His intrusive thoughts may lead to attempts to suppress those thoughts and, eventually, to exacerbated negative mood.
- His negative mood and preoccupation with thoughts of discovery may subsequently cause him to behave awkwardly at the reunion, especially when extended family members ask him if he has a girlfriend.
- His awkwardly avoidant response (or outright lie) may cause him to see himself and his stigma negatively, which may also adversely impact his subsequent cognitive, affective, and behavioral functioning.
- He may seek to avoid similar situations in the future, a strategy that may also impair his mental health and family relationships and is likely to preclude efficacious interactions with his environment.
Disclosure of his stigma could potentially interrupt this cycle and bring him to a higher level of functioning, but disclosure can also come at a cost.
How to Break the Cycle
There are excellent reviews of the costs and benefits to be weighed in deciding whether to reveal potentially stigmatizing information
- (e.g., Derlega & Berg, 1987; K. Greene et al. 2003; Holmes & River, 1998; Kelly & McKillop, 1996; Larson & Chastain, 1990).
Beyond deciding whether to disclose a stigma on the basis of an analysis of these costs and benefits, however, individuals with a concealable stigma can consider breaking the distressing cycle at any place along the route depicted in Figure 1.
Appropriately attributing negative psychological outcomes to concealing a stigma, instead of to personal flaws or deficiencies, can alleviate some of the distress experienced by stigmatized individuals (Miller & Major, 2000).
It is important to make such reattributions only in situations in which this is appropriate and only in the presence of clear situational cues that negative outcomes are a likely result of stigma-related difficulties (Miller & Major, 2000).
The gay teenager in the above example, for instance, can reattribute his awkward behavior in his interaction with his extended family as a necessary response to their unfortunate insensitivity, their obliviousness to the range of possible sexual orientations, or their possible bias against nonheterosexual identities. Reattributing distress to the difficulties associated with hiding a key attribute of oneself may enable some individuals with a concealable stigma to see that they are not flawed or otherwise deficient. In the present model, self-evaluation allows such a reattribution to positively impact subsequent thoughts, feelings, and behavior as well as the nature of future situations.
Individuals with a concealable stigma may elect to selectively disclose their stigmatized status to safe others. Numerous studies have supported the notion that emotional or personal self-disclosure can be positively associated with mental well-being (e.g., Jourard, 1971; Pennebaker, Kiecolt-Glaser, & Glaser, 1988).
For decades, many have proffered theories of the self-esteem boost that results from self-disclosure. The early writings of the symbolic interactionists (e.g., Cooley, 1902/1922; Dewey, 1922; Mead, 1934) postulated that people form their self-concepts through their interactions with others and that positive interactions lead to positive self-concepts. In the early 1970s Jourard (1971) proposed that an individual forms a positive self-concept only when presenting his or her true self to others. In presenting his or her true self, the individual receives genuine feedback about that self — feedback that contributes to the formation of an authentic self-concept. Jourard postulated that only in presenting one’s true self can an individual become fully known to others and, thus, to oneself.
Individuals who conceal a stigma may be cut off from genuine social interactions in which feedback helps establish a positive self-concept. They may note the discrepancy between their true self and the self that they present to others, resulting in feelings of inauthenticity, as if they are living a lie. The more central one’s stigmatized status is to one’s self-concept, the more threatening a lack of feedback may be to the eventual development of a positive sense of self.
More recent evidence has suggested that disclosure of a stigmatized identity is associated with (and may indeed lead to) greater self-acceptance.
In one study, disclosing about the lesbian identity of one’s mother was correlated with higher self-esteem in a sample of 76 adolescent children of lesbian mothers (Gershon, Tschann, & Jemerin, 1999). Similarly, gay men who have disclosed their sexual orientation to their mothers have higher self-esteem (Savin-Williams, 1989).
Herek (2003) explained why self-disclosure of one’s nonheterosexual orientation may be beneficial. Specifically, he suggested that because nonheterosexual orientations are often highly stigmatizing in U.S. society, disclosing one’s nonheterosexual orientation can be personally affirming and is an important part of self-acceptance and forming a positive identity. The present model suggests that this more positive self-evaluation occurs as a result of the positive feedback that one may receive upon disclosure. This particular process is highlighted by the disclosure – feedback–self-evaluation link depicted in Figure 1.
Empirical evidence supports this link. Specifically, participation in an online message group in one study led to greater importance of a stigmatized identity for those with stigmatized sexual identities or sociopolitical ideologies. This increased stigma importance, in turn, led to greater self-acceptance and a higher likelihood of coming out to family and friends about this identity (McKenna & Bargh, 1998).
This suggests that when people with a concealable stigma receive positive feedback about their stigma, they are more motivated to bring their hidden selves in line with their presented selves. For some time now, others have noted that congruity between private and public selves is associated with feelings of self-worth and self-esteem (e.g., Baumeister, 1982). Because of this, it is very likely that despite its costs, disclosing can alleviate the difficulties inherent in hiding, especially hiding a core aspect of one’s identity.
However, it is important to keep in mind that concealment often serves as an adaptation to hostile environments. Individuals with a concealable stigma may wish to choose a realistic placement of boundaries in the disclosure–concealment continuum while recognizing the functional nature of concealment. In doing so, they must consider the support that they are likely to receive from various others.
Individuals who plan to disclose any secret may benefit from considering various qualities of confidants that may predict their reaction to being told stigmatizing information (Kelly, 2002). Specifically, Kelly (2002) suggests considering a confidant’s perceived discreetness and the likelihood that they will negatively evaluate or reject the person who discloses.
In fact, evidence suggests that telling a nonsupportive other can lead to poorer well-being than telling no one at all. Those women who told close others about a recent abortion but perceived them to be less than supportive of this information adjusted more poorly to their abortion than did women who did not tell or women who told another person whom they perceived to be supportive (Major et al., 1990).
Clearly, individuals who have a concealable stigma must carefully evaluate the possible consequences of disclosing to others.
Earlier, this article highlighted the features of situations that are likely to lead to negative psychological consequences in the proposed model. It should also be noted that certain situational features are likely to produce positive psychological consequences.
For instance, the presence of similar others, though it increases the salience of one’s stigma, is not likely to be associated with negative psychological consequences. In fact, evidence suggests that the presence of similar others can have beneficial outcomes for individuals with a concealable stigma.
For example, students who were gay, bulimic, or from a working class background reported more positive mood and increased self-esteem when in the presence of similar others (Frable et al., 1998). Probably because of the concealable nature of their stigma, however, these students were less likely than students with a visible stigma to be in such situations.
The presence of positive cues may also promote positive psychological consequences. For example, the presence of gay-pride symbols convey acceptance and support and are likely to lead to feelings of comfort for a gay person. When such situational features are present, individuals may feel less compelled to hide and thus less hampered by the negative consequences of hiding.
Individuals who similarly share a concealable stigma reflect for each other the challenges involved in negotiating an identity that is complicated by both stigma and concealability. Individuals who conceal a stigma may have always perceived their stigma as worthy of being hidden. Encounters with similar others offer concealing individuals the opportunity to present their more genuine selves — stigma and all — and to incorporate the feedback that accrues from that more genuine self-presentation into a more positive overall view of oneself.
In addition, contact with similar others allows for the eventual cognitive reattribution of the source of one’s distress (through feedback from similar others and its subsequent impact on self-evaluation). This reattribution is preferable to attributing one’s distress to the possession of a stigma, per se, as may occur in the absence of contact with similar others (see the link between self-evaluative implications and cognitive, affective, and behavioral implications in Figure 1).
Although the model focuses on the negative process of concealing a stigma, one can also use the model to understand the positive process of disclosing a stigma. According to the model, positive feedback toward more genuine behavior will lead to more positive self-evaluations. These improved self-evaluations will not only lead to more positive cognitions and affect but will also increase the likelihood that the individual will enter more risky situations in the future (e.g., disclosing to nonsimilar others). Success in these situations will result in more positive cognitive, affective, and behavioral outcomes in a cyclical, self-perpetuating manner.
Through examination of Figure 1, it is clear that disclosing in these situations changes the nature of the situation. Specifically, once an individual discloses and receives positive feedback, he or she is likely to hold a more efficacious view of his or her ability to succeed in such situations in the future. Of course, if positive feedback is not forthcoming, the positive self-evaluative consequences of disclosure and the subsequent willingness to take the risk of future disclose may decrease. This may maintain the negative cycle. Yet, clinical experience suggests that once a critical mass of success experiences has accrued, an individual’s positive self-evaluation may be sufficiently strong to prevent reentry into the negative cycle (e.g., Bandura, 1977; Goldfried & Robins, 1982). Part of this process is highlighted in Figure 1 as the disclosure–feedback–self-evaluative implications link.
Summary of Different Implications of Concealable Versus Visible Stigmas
The psychological consequences reviewed above and the process that links them differs from the consequences and process of possessing a visible stigma. The cognitive–affective–behavioral path in the present model may operate similarly for individuals who possess concealable and visible stigmas. However, some of the other pathways in the model, as well as the operation of the process as a whole, may be unique to individuals with a concealable stigma for three reasons.
First, individuals who conceal a stigma can never fully internalize feedback from others as feedback about one’s genuine self (i.e., the disclosure–feedback link in Figure 1).
Second, individuals who conceal a stigma forfeit the benefits of protection provided by other stigmatized group members. As a result, cognitive reattribution for one’s stigma-related difficulties cannot readily occur, thereby leaving the individual to assume personal responsibility for his or her distress (i.e., the bidirectional links from self-evaluative implications in Figure 1).
Third, distress occurs not only from the consequences of possessing a stigma but also from the fears that the stigma will be discovered and punished. The impact of this fear of discovery on behaviors such as avoidance is unique to concealing a stigma (i.e., the link from affective implications to behavioral implications in Figure 1).
Further, according to the research reviewed in previous sections, it seems that the consequences within each domain (cognitive, affective, behavioral, self-evaluative) differ for individuals with a concealable versus a visible stigma.
Whereas individuals with any type of stigma, concealable or visible, may experience preoccupation, vigilance, and suspiciousness, individuals with a concealable stigma are more likely to be preoccupied with giving off clues of the stigma, vigilant of the possibility that the stigma is suspected, and suspicious that their stigma has been discovered.
Individuals with a visible stigma are probably less concerned about disclosing a secret and more concerned that their obvious stigma is interfering with a given interaction. Although many individuals who face a situational challenge, stigma related or not, may share the affective implications discussed in this model (i.e., shame, fear of negative evaluation, anxiety, depression, hostility, demoralization, guilt), these implications are likely to be of a different quality when they result from hiding a more-or-less core aspect of one’s identity.
For example, many individuals may doubt that they can convey a desired impression of themselves and therefore expect negative evaluation in a particular situation. However, individuals with a concealable stigma may doubt that they can hide the stigmatized aspects of themselves and thus expect the negative evaluative consequences of being found out in that situation.
The behavioral consequences of stigma also seem particularly likely to differ depending on whether the stigma is concealable or visible.
For example, although people with either type of stigma may attempt to manage the impressions they convey, individuals with a visible stigma are not likely to be concerned with giving off the impression that they are stigmatized, because this is an obvious fact in nearly all of their social interactions. Similarly, individuals with a concealable stigma are likely to avoid social situations because they fear that someone will discover their stigma and subsequently reject, ridicule, or discriminate against them.
In addition, however, these individuals may experience close relationship impairment as a result of the cognitive and affective distress that accompanies hiding an important part of their identity. As individuals with an obvious stigma cannot hide their stigma, their social functioning is not similarly impacted. Also, once they disclose their stigmatized identity, individuals with a concealable stigma are likely to attach significant importance to the feedback that they receive from others given the relative infrequency of its occurrence. Individuals with a visible stigma probably do not attach as much importance to every individual instance of feedback about their stigma, given the high frequency of such feedback, whether actual or only perceived.
Finally, the self-evaluative consequences of possessing a stigma differ in a number of ways depending on whether the stigma is hidden or concealed. Whereas individuals with a visible stigma may see themselves negatively for possessing a stigma, individuals with a concealable stigma may see themselves negatively not only for possessing the stigma but also for keeping it hidden.
Further, when an individual hides a stigma, he or she cannot access positive feedback from other members of the group. The absence of this feedback may be associated with an overall view of oneself into which one’s stigma is not fully integrated. Individuals with a concealable stigma may also lack the efficacy to change their stigma-related difficulties through disclosure to others.
The findings reviewed above do not prove that concealing a stigma is any more distressing than contending with a visible stigma. However, these findings and the proposed model that incorporates them do seem to challenge the expectation of Jones et al. (1984) that “individuals who have concealed marks would be better adjusted than people whose blemish is apparent” (p. 35). Of course, to more solidly test this claim, researchers must examine the unique difficulties of concealing a stigma as well as the specific pathways that link these difficulties in the proposed model, as discussed next.
Future Research Directions
Researchers have found higher rates of psychopathology for individuals with concealable stigmas compared with the general population
- (e.g., Cochran, Greer Sullivan, & Mays, 2003; Cochran & Mays, 2000; Gilman et al., 2001; Herrell et al., 1999; Sandfort, de Graaf, Bijl, & Schnabel, 2001).
Lest one conclude that these higher rates are attributable to the stigma itself (as has been done for homosexuality, see e.g., Cameron & Cameron, 1998), the process model established here strongly suggests that the hidden dimension of stigma impairs the psychological functioning of individuals with a concealable stigma. In fact, recent conceptualizations of minority stress suggest that concealability may contribute unique variance to the overall functioning of stigmatized individuals (Meyer, 2003).
Basic research in many areas of psychology support the process of the model proposed here.
Personality researchers have established that elements of a situation at least partially determine people’s behavior in that situation
- (e.g., Bem & Allen, 1974; Bowers, 1973; Ekehammar, 1974; Mischel, 1973; Mischel & Shoda, 1995).
Experimental data also show that cognitive elements, such as an individual’s perception of a situation, mediate the situation–behavior link (e.g., Meichenbaum, 1972) and that cognition and affect impact each other in a bidirectional fashion
- (e.g., Bower, 1981; Schachter & Singer, 1962; Teasdale & Russell, 1983).
Further, experimental data clearly support the notion that an individual’s self-evaluation impacts his or her behavior, cognition, and affect and that these psychological domains, in turn, impact self-evaluation
- (e.g., Bandura, 1988; Bandura & Adams, 1977; Bandura et al., 1988; Bandura, Reese, & Adams, 1982; Cervone et al., 1994; Harackiewicz, Sansone, & Manderlink, 1985; Salovey & Birnbaum, 1989).
Taken together, this research suggests that a cognitive–affective–behavioral–self-evaluation process exists in response to general goals.
Researchers now face the task of determining whether this process operates for individuals who have the specific goal of concealing a stigma in stigma-related situations. In fact, some of the studies reviewed in this article have already begun this task.
Although many of the studies reviewed here simply establish the association between concealing a stigma and experiencing impairment in one of the general domains (i.e., cognition, affect, behavior, self-evaluation), some of these studies directly support the proposed links of this model.
For example, the study by Kalichman and Nachimson (1999) suggested possible links between low self-efficacy, risky behavior, and affective distress for people who conceal their HIV-positive status. In addition, the studies by Major and Gramzow (1999) and Beals (2004) offer evidence that one process (e.g., active suppression of information about one’s concealable stigma) may lead to other specific consequences (e.g., greater psychological distress) in the model.
More research such as this, with possible mediation analyses (e.g., suppression leads to distress as a result of stigma-related thought intrusion), will further support the proposed model. Preliminary evidence also suggests that socializing with similarly stigmatized others may be a potentially important way to break the distress cycle by increasing positive affect and self-evaluation (Frable et al., 1998).
More research needs to focus on the currently untested links between concealing a stigma and experiencing specific components (e.g., preoccupation, anxiety, avoidance, low self-efficacy) of each broad domain (i.e., cognition, affect, behavior, self-evaluation) of the model.
For example, researchers need to test the proposition that individuals with a concealable stigma may evince higher self-monitoring than do individuals without a concealable stigma. Unfortunately, it is difficult to recruit large numbers of participants who hide the characteristic that qualifies them for participation in these studies. Still, some researchers have proposed unique recruitment methods that, although costly, have the potential to increase the feasibility of this task (e.g., Watters & Biernacki, 1989).
Because studies rarely include both visible and concealable stigmas and because it is difficult to manipulate whether a stigma is visible or concealable, one cannot unequivocally determine which consequences are unique to concealable stigmas. Taken together, though, the studies reviewed in this article suggest that there are unique consequences of possessing a concealable stigma that are not necessarily shared by individuals who possess a visible stigma.
The study by Frable et al. (1998) is ideal in that it directly compared the experiences of individuals with concealable and visible stigmas, finding that students with concealable stigmas reported lower self-esteem and more negative affect.
Further, the study by Santuzzi and Ruscher (2002) took the novel approach of randomly assigning participants to role play the experience of possessing a concealable stigma in order to approximate the psychological experience of concealing a stigma from others. Somewhat similarly, Smart and Wegner (1999) cleverly asked women with and without an eating disorder to role play either having or not having an eating disorder in order to manipulate the visibility or concealability of that stigma. The researchers then determined differences in the degree of cognitive interference in each of the two groups. This area needs more studies using creative designs like these to examine other unique implications of concealing a stigma.
Although not included in the present model, research supports the notion that the negative psychological consequences of concealing a stigma may lead to poorer physical health. The stress of inhibiting emotional expression has been shown to lead to negative physical health consequences
- (e.g., Pennebaker, Kiecolt-Glaser, & Glaser, 1988; Richards, Beal, Seagal, & Pennebaker, 2000).
In addition, disclosing traumatic experiences or personal information about oneself has been shown to improve health functioning through the alleviation of the anxiety and distress that accompanies hiding this information (Bucci, 1995; Stiles, 1995).
Two studies provide convincing evidence that concealing a stigmatized identity, in particular, may lead to negative physical health outcomes.
Both studies examined the physical health of gay men who concealed their sexual identity and found that these men were significantly more susceptible to infectious diseases and impaired immunological functioning than were those who did not conceal their gay identity
- (Cole, Kemeny, Taylor, & Visscher, 1996; Ullrich, Lutgendorf, & Stapleton, 2003).
Although comparable data do not exist for individuals with other concealable stigmas, these studies offer evidence that concealing a core aspect of oneself may be associated with negative physical health consequences. More work such as this would strengthen the claim that concealing a stigma not only requires much mental work but can also take its toll on physical health.
Over 40 years ago, Goffman (1963) offered preliminary evidence drawn from autobiographies and case studies that suggested that concealing a stigma may be fraught with unique challenges. Since that time, increasing empirical evidence has substantiated Goffman’s observation. This article offers a framework from which to examine that evidence and from which to consider the routes by which individuals can overcome the difficulties inherent in concealing a stigma.
Remark
I thank Lisa Burckell, Catherine Eubanks-Carter, Marvin Goldfried, Daniel Klein, and Sheri Levy for their very helpful feedback on earlier versions of this article.
References
Andersen, S. M., & Chen, S. (2002). The relational self: An interpersonal social-cognitive theory. Psychological Review, 109, 619 – 645.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84, 194 –215.
Bandura, A. (1988). Self-efficacy conception of anxiety. Anxiety Research, 1, 77–98.
Bandura, A., & Adams, N. E. (1977). Analysis of self-efficacy theory of behavioral change. Cognitive Therapy and Research, 1, 287–310.
Bandura, A., Adams, N. E., & Beyer, J. (1977). Cognitive processes mediating behavioral change. Journal of Personality and Social Psychology, 35, 125–139.
Bandura, A., Cioffi, D., Taylor, C. B., & Brouillard, M. E. (1988). Perceived self-efficacy in coping with cognitive stressors and opioid activation. Journal of Personality and Social Psychology, 55, 479 – 488.
Bandura, A., Reese, L., & Adams, N. E. (1982). Micro-analysis of action and fear arousal as a function of differential levels of perceived self-efficacy. Journal of Personality and Social Psychology, 43, 5–21.
Baumeister, R. F. (1982). Self-esteem, self-presentation, and future interaction: A dilemma of reputation. Journal of Personality, 50, 29 – 45.
Beals, K. P. (2004). Stigma management and well-being: The role of social support, cognitive processing, and suppression. Dissertation Abstracts International, 65 (02), 1070B. (UMI No. 3121250) Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York: International Universities Press.
Bem, D. (1972). Self-perception theory. In L. Berkowitz (Ed.), Advances in experimental social psychology (Vol. 6, pp. 1–62). San Diego, CA: Academic Press.
Bem, D. J., & Allen, A. (1974). On predicting some of the people some of the time: The search for cross-situational consistencies in behavior. Psychological Review, 81, 506 –520.
Bower, G. H. (1981). Mood and memory. American Psychologist, 36, 129 –148.
Bowers, K. S. (1973). Situationism in psychology: An analysis and critique. Psychological Review, 80, 307–336.
Bucci, W. (1995). The power of the narrative: A multiple code account. In J. W. Pennebaker (Ed.), Emotion, disclosure, & health (pp. 93–122). Washington, DC: American Psychological Association.
Burgoon, J. K., & Buller, D. B. (1994). Interpersonal deception: III. Effects of deceit on perceived communication and nonverbal behavior dynamics. Journal of Nonverbal Behavior, 18, 155–184.
Burns, R. B. (1979). The self-concept: In theory, measurement, development, and behavior. London: Longman.
Cain, R. (1991). Stigma management and gay identity development. Social Work, 36, 67–73.
Cameron, P., & Cameron, K. (1998). Homosexual parents: A comparative forensic study of character and harms to children. Psychological Reports, 82, 1155–1191.
Cepeda-Benito, A., & Short, P. (1998). Self-concealment, avoidance of psychological services, and perceived likelihood of seeking professional help. Journal of Counseling Psychology, 45, 58 – 64.
Cervone, D., Kopp, D. A., Schaumann, L., & Scott, W. D. (1994). Mood, self-efficacy, and performance standards: Lower moods induce higher standards for performance. Journal of Personality and Social Psychology, 67, 499 –512.
Chanowitz, B., & Langer, E. J. (1981). Premature cognitive commitment. Journal of Personality and Social Psychology, 41, 1051–1063.
Chesney, M. A., & Smith, A. W. (1999). Critical delays in HIV testing and care: The potential role of stigma. American Behavioral Scientist, 42, 1162–1174.
Clair, J. A., Beatty, J. E., & MacLean, T. L. (2005). Out of sight but not out of mind: Managing invisible social identities in the workplace. Academy of Management Review, 1, 78 –95.
Clark, R., Anderson, N. B., Clark, V. R., & Williams, D. R. (1999). Racism as a stressor for African Americans: A biopsychosocial model. American Psychologist, 54, 805– 816.
Cochran, S. D., Greer Sullivan, J., & Mays, V. M. (2003). Prevalence of mental disorders, psychological distress, and mental health services use among lesbian, gay, and bisexual adults in the United States. Journal of Consulting and Clinical Psychology, 71, 53– 61.
Cochran, S. D., & Mays, V. M. (2000). Lifetime prevalence of suicide symptoms and affective disorders among men reporting same-sex sexual partners: Results from NHANES III. American Journal of Public Health, 90, 573–578.
Cole, S. W., Kemeny, M. E., Taylor, S. E., & Visscher, B. R. (1996). Elevated physical health risk among gay men who conceal their homosexual identity. Health Psychology, 15, 243–251.
Comer, L. K., Henker, B., Kemeny, M., & Wyatt, G. (2000). Illness disclosure and mental health among women with HIV/AIDS. Journal of Community & Applied Social Psychology, 10, 449 – 464.
Cooley, C. H. (1922). Human nature and the social order. New York: Scribner. (Original work published 1902)
Corrigan, P. W., & Kleinlein, P. (2005). The impact of mental illness stigma. In P. W. Corrigan (Ed.), On the stigma of mental illness: Practical strategies for research and social change (pp. 11–44). Washington, DC: American Psychological Association.
Corrigan, P. W., & Matthews, A. K. (2003). Stigma and disclosure: Implications for coming out of the closet. Journal of Mental Health, 12, 235–248.
Cozby, P. C. (1972). Self-disclosure, reciprocity and liking. Sociometry, 35, 151–160.
Cramer, K. M., & Lake, R. P. (1998). The Preference for Solitude Scale: Psychometric properties and factor structure. Personality and Individual Differences, 24, 193–199.
Crocker, J., & Major, B. (1989). Social stigma and self-esteem: The self-protective properties of stigma. Psychological Review, 96, 608 – 630.
Crocker, J., Major, B., & Steele, C. (1998). Social stigma. In D. T. Gilbert [[PAGE_342]] & S. T. Fiske (Eds.), Handbook of social psychology (4th ed., Vol. 2, pp. 504–553). Boston: McGraw-Hill.
Crocker, J., & Quinn, D. M. (2000). Social stigma and the self: Meanings, situations, and self-esteem. In T. F. Heatherton & R. E. Kleck (Eds.), Social psychology of stigma (pp. 153–183). New York: Guilford Press.
Croteau, J. M. (1996). Research on the work experiences of lesbian, gay, and bisexual people: An integrative review of methodology and findings. Journal of Vocational Behavior, 48, 195–209.
DePaulo, B. M. (1992). Nonverbal behavior and self-presentation. Psychological Bulletin, 111, 203–243.
DePaulo, B. M., Ansfield, M. E., Kirkendol, S. E., & Boden, J. M. (2004). Serious lies. Basic and Applied Social Psychology, 26, 147–167.
Derlega, V. J., & Berg, J. H. (1987). Self-disclosure: Theory, research, and therapy. New York: Plenum Press.
Derlega, V. J., Metts, S., Petronio, S., & Margulis, S. T. (1993). Self-disclosure. Thousand Oaks, CA: Sage.
Dewey, J. (1922). Human nature and conduct. New York: Modern Library.
Dion, K. L. (2002). The social psychology of perceived prejudice and discrimination. Canadian Psychology, 43, 1–10.
Dohrenwend, B. P. (2000). The role of adversity and stress in psychopathology: Some evidence and its implications for theory and research. Journal of Health and Social Behavior, 41, 1–19.
Downey, G., & Feldman, S. I. (1996). Implications of rejection sensitivity for intimate relationships. Journal of Personality and Social Psychology, 70, 1327–1343.
Dweck, C. S., & Leggett, E. L. (1988). A social-cognitive approach to motivation and personality. Psychological Review, 95, 256 –273.
Ekehammar, B. (1974). Interactionism in personality from a historical perspective. Psychological Bulletin, 81, 1026 –1048.
Endler, N. S., & Bain, J. M. (1966). Interpersonal anxiety as a function of social class. Journal of Social Psychology, 70, 221–227.
Endler, N. S., Hunt, J. M., & Rosenstein, A. J. (1962). An S-R inventory of anxiousness. Psychological Monographs, 76, 33.
Epstein, S. (1979). The stability of behavior: On predicting most of the people much of the time. Journal of Personality and Social Psychology, 37, 1097–1126.
Epstein, S., & Erskine, N. (1983). The development of personal theories of reality. In D. Magnusson & V. Allen (Eds.), Human development: An interactional perspective (pp. 133–147). New York: Academic Press.
Farina, A., Gliha, D., Boudreau, L. A., Allen, J. G., & Sherman, M. (1971). Mental illness and the impact of believing others know about it. Journal of Abnormal Psychology, 77, 1–5.
Federal Bureau of Investigation. (2004). Hate crime statistics 2003. Retrieved August 1, 2005, from http://www.fbi.gov/ucr/03hc.pdf
Fishbein, M. J., & Laird, J. D. (1979). Concealment and disclosure: Some effects of information control on the person who controls. Journal of Experimental Social Psychology, 15, 114 –121.
Frable, D. E. S., Blackstone, T., & Scherbaum, C. (1990). Marginal and mindful: Deviants in social interactions. Journal of Personality and Social Psychology, 59, 140 –149.
Frable, D. E. S., Platt, L., & Hoey, S. (1998). Concealable stigmas and positive self-perceptions: Feeling better around similar others. Journal of Personality and Social Psychology, 74, 909 –922.
Frable, D. E. S., Wortman, C., & Joseph, J. (1997). Predicting self-esteem, well-being, and distress in a cohort of gay men: The importance of cultural stigma, personal visibility, community networks, and positive identity. Journal of Personality, 65, 599 – 624.
Freeman, H. E., & Kassebaum, G. G. (1956). The illiterate in American society: Some general hypotheses. Social Forces, 34, 371–375.
Gershon, T. D., Tschann, J. M., & Jemerin, J. M. (1999). Stigmatization, self-esteem, and coping among the adolescent children of lesbian mothers. Journal of Adolescent Health, 24, 437– 445.
Gesell, S. B. (1999). The roles of personality and cognitive processing in secret-keeping. Dissertation Abstracts International, 60 (06), 2971B. (UMI No. 9935342)
Gilman, S. E., Cochran, S. D., Mays, V. M., Hughes, M., Ostrow, D., & Kessler, R. C. (2001). Risk of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Survey. American Journal of Public Health, 91, 933–939.
Goffman, E. (1963). Stigma: Notes on the management of a spoiled identity. Englewood Cliffs, NJ: Prentice Hall.
Goldfried, M. R. (1995). Toward a common language for case formulation. Journal of Psychotherapy Integration, 5, 221–244.
Goldfried, M. R., & Goldfried, A. P. (2001). The importance of parental support in the lives of gay, lesbian, and bisexual individuals. Journal of Clinical Psychology, 57, 681– 693.
Goldfried, M. R., & Robins, C. J. (1982). On the facilitation of self-efficacy. Cognitive Therapy and Research, 6, 361–380.
Granfield, R. (1991). Making it by faking it: Working-class students in an elite academic environment. Journal of Contemporary Ethnography, 20, 331–351.
Greene, J. O., O’Hair, H. D., Cody, M. J., & Yen, C. (1985). Planning and control of behavior during deception. Human Communication Research, 11, 335–364.
Greene, K., Derlega, V. J., Yep, G. A., & Petronio, S. (2003). Privacy and disclosure of HIV in interpersonal relationships: A sourcebook for researchers and practitioners. Mahwah, NJ: Erlbaum.
Halverson, C. F. J., & Shore, R. E. (1969). Self-disclosure and interpersonal functioning. Journal of Consulting and Clinical Psychology, 33, 213–217.
Harackiewicz, J., Sansone, C., & Manderlink, G. (1985). Competence, achievement orientation, and intrinsic motivation: A process analysis. Journal of Personality and Social Psychology, 48, 493–508.
Harvey, J. H., & Wenzel, A. (2002). HIV, AIDS, and close relationships. Journal of Social and Personal Relationships, 19, 135–142.
Hebl, M. R., Tickle, J., & Heatherton, T. F. (2000). Awkward moments in interactions between nonstigmatized and stigmatized individuals. In T. F. Heatherton & R. E. Kleck (Eds.), Social psychology of stigma (pp. 275–306). New York: Guilford Press.
Heckman, T. G., Anderson, E. S., Sikkema, K. J., Kochman, A., Kalichman, S. C., & Anderson, T. (2004). Emotional distress in nonmetropolitan persons living with HIV disease enrolled in a telephone-delivered, coping improvement group intervention. Health Psychology, 23, 94 – 100.
Herek, G. M. (1998). Stigma and sexual orientation: Understanding prejudice against lesbians, gay men, and bisexuals. Newbury Park, CA: Sage.
Herek, G. M. (1999). AIDS and stigma. American Behavioral Scientist, 42, 1106 –1116.
Herek, G. M. (2003). Why tell if you’re not asked? Self-disclosure, intergroup contact, and heterosexuals’ attitudes toward lesbians and gay men. In L. D. Garnets & D. C. Kimmel (Eds.), Psychological perspectives on lesbian, gay, and bisexual experiences (2nd ed., pp. 270–298). New York: Columbia University Press.
Herek, G. M., & Berrill, K. T. (1992). Hate crimes: Confronting violence against lesbians and gay men. Newbury Park, CA: Sage.
Herek, G. M., Gillis, J. R., & Cogan, J. C. (1999). Psychological sequelae of hate-crime victimization among lesbian, gay, and bisexual adults. Journal of Consulting and Clinical Psychology, 67, 945–951.
Herman, N. J. (1993). Return to sender: Reintegrative stigma-management strategies of ex-psychiatric patients. Journal of Contemporary Ethnography, 22, 295–330.
Herrell, R., Goldberg, J., True, W. R., Ramakrishnan, V., Lyons, M., Eisen, S., et al. (1999). Sexual orientation and suicidality: A co-twin control study in adult men. Archives of General Psychiatry, 56, 867– 874.
Hershberger, S. L., & D’Augelli, A. R. (1995). The impact of victimization [[PAGE_343]] on the mental health and suicidality of lesbian, gay, and bisexual youths. Developmental Psychology, 31, 65–74.
Hetrick, E. S., & Martin, A. D. (1987). Developmental issues and their resolution for gay and lesbian adolescents. Journal of Homosexuality, 14, 25– 43.
Hétu, R. (1996). The stigma attached to hearing impairment. Scandinavian Audiology Supplement, 25, 12–24.
Higgins, P. O. (1980). Outsiders in a hearing world: A sociology of deafness. Beverly Hills, CA: Sage.
Holmes, P. E., & River, L. P. (1998). Individual strategies for coping with the stigma of severe mental illness. Cognitive and Behavioral Practice, 5, 231–239.
Ichiyama, M. A., Colbert, D., Laramore, H., & Heim, M. (1993). Self-concealment and correlates of adjustment in college students. Journal of College Student Psychotherapy, 7, 55– 68.
Jones, E. E., Farina, A., Hastorf, A. H., Markus, H., Miller, D. T., & Scott, A. S. (1984). Social stigma: The psychology of marked relationships. New York: Freeman.
Jourard, S. M. (1971). Self-disclosure: An experimental analysis of the transparent self. New York: Wiley.
Kalichman, S. C., & Nachimson, D. (1999). Self-efficacy and disclosure of HIV-positive serostatus to sex partners. Health Psychology, 18, 281– 287.
Kelly, A. E. (1998). Clients’ secret keeping in outpatient therapy. Journal of Counseling Psychology, 45, 50 –57.
Kelly, A. E. (2002). The psychology of secrets. New York: Kluwer Academic/Plenum.
Kelly, A. E., & Kahn, J. H. (1994). Effects of suppression of personal intrusive thoughts. Journal of Personality and Social Psychology, 66, 998 –1006.
Kelly, A. E., & McKillop, K. J. (1996). Consequences of revealing personal secrets. Psychological Bulletin, 120, 450 – 465.
Kessler, R. C., Mickelson, K. D., & Williams, D. R. (1999). The prevalence, distribution, and mental health correlates of perceived discrimination in the United States. Journal of Health and Social Behavior, 40, 208 –230.
Kessler, R. C., & Neighbors, H. W. (1986). A new perspective on the relationships among race, social class, and psychological distress. Journal of Health and Social Behavior, 27, 107–115.
King, L. A., Emmons, R. A., & Woodley, S. (1992). The structure of inhibition. Journal of Research in Personality, 26, 85–102.
Kleck, R. D. (1968). Self-disclosure patterns of the nonobviously stigmatized. Psychological Reports, 23, 1239 –1248.
Koss, M. P. (1985). The hidden rape victim: Personality, attitudinal, and situational characteristics. Psychology of Women Quarterly, 9, 193–212.
Lane, J. D., & Wegner, D. M. (1995). The cognitive consequences of secrecy. Journal of Personality and Social Psychology, 69, 237–253.
Lange, T. (2003, November). HIV & civil rights: A report from the frontlines of the HIV/AIDS epidemic. Retrieved August 1, 2005, from American Civil Liberties Union Web site: http://www.aclu.org/pdfs/ hivaids/hiv_civilrights.pdf
Langer, E. J. (1989). Mindfulness. Reading, MA: Addison Wesley.
Langer, E. J., & Piper, A. I. (1987). The prevention of mindlessness. Journal of Personality and Social Psychology, 53, 280 –287.
Larson, D. G., & Chastain, R. L. (1990). Self-concealment: Conceptualization, measurement, and health implications. Journal of Social & Clinical Psychology, 9, 439 –455.
Lee, J. D., & Craft, E. A. (2002). Protecting one’s self from a stigmatized disease . . . once one has it. Deviant Behavior, 23, 267–299.
Letkemann, P. (2002). Unemployed professionals, stigma management and derivative stigmata. Work, Employment and Society, 16, 511–522.
Lévy, A., Laska, F., Abelhauser, A., Delfraissy, J.-F., Goujard, C., Boué, F., et al. (1999). Disclosure of HIV seropositivity. Journal of Clinical Psychology, 55, 1041–1049.
Link, B. G., Mirotznik, J., & Cullen, F. T. (1991). The effectiveness of stigma coping orientations: Can negative consequences of mental illness labeling be avoided? Journal of Health and Social Behavior, 32, 302– 320.
Magnusson, D. (1990). Personality development from an interactional perspective. In L. A. Pervin (Ed.), Handbook of personality: Theory and research (pp. 193–124). New York: Guilford Press.
Major, B., Cozzarelli, C., Sciacchitano, A. M., Cooper, M. L., Testa, M., & Mueller, P. M. (1990). Perceived social support, self-efficacy, and adjustment to abortion. Journal of Personality and Social Psychology, 59, 452– 463.
Major, B., & Gramzow, R. H. (1999). Abortion as stigma: Cognitive and emotional implications of concealment. Journal of Personality and Social Psychology, 77, 735–745.
Markus, H., & Wurf, E. (1987). The dynamic self-concept: A social psychological perspective. Annual Review of Psychology, 38, 299 –337.
Matthews, C. K., & Harrington, N. G. (2000). Invisible disability. In D. O. Braithwaite & T. L. Thompson (Eds.), Handbook of communication and people with disabilities: Research and application (pp. 405–421). New York: Erlbaum.
McKenna, K. Y. A., & Bargh, J. A. (1998). Coming out in the age of the internet: Identity “demarginalization” through virtual group participation. Journal of Personality and Social Psychology, 75, 681– 694.
Mead, G. H. (1934). Mind, self, and society. Chicago: University of Chicago Press.
Meichenbaum, D. (1972). Cognitive modification of test anxious college students. Journal of Consulting and Clinical Psychology, 39, 370 –380.
Mendoza-Denton, R., Downey, G., Purdie, V. J., Davis, A., & Pietrzak, J. (2002). Sensitivity to status-based rejection: Implications for African American students’ college experience. Journal of Personality and Social Psychology, 83, 896 –918.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674 – 697.
Miall, C. E. (1986). The stigma of involuntary childlessness. Social Problems, 33, 268 –282.
Miller, C. T., & Major, B. (2000). Coping with stigma and prejudice. In T. F. Heatherton & R. E. Kleck (Eds.), Social psychology of stigma (pp. 243–272). New York: Guilford Press.
Mischel, W. (1973). Toward a cognitive social learning theory reconceptualization of personality. Psychological Review, 80, 252–283.
Mischel, W., & Shoda, Y. (1995). A cognitive–affective system theory of personality: Reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychological Review, 102, 246 – 268.
Murphy, D. A., Roberts, K. J., & Hoffman, D. (2002). Stigma and ostracism associated with HIV/AIDS: Children carrying the secret of their mothers’ HIV+ serostatus. Journal of Child and Family Studies, 11, 191–202.
Nicholson, W. D., & Long, B. C. (1990). Self-esteem, social support, internalized homophobia, and coping strategies of HIV+ gay men. Journal of Consulting and Clinical Psychology, 58, 873– 876.
North, R. L., & Rothenberg, K. H. (1993). Partner notification and the threat of domestic violence against women with HIV infection. New England Journal of Medicine, 329, 1194 –1196.
Olney, M. F., & Brockelman, K. F. (2003). Out of the disability closet: Strategic use of perception management by select university students with disabilities. Disability & Society, 18, 35–50.
Pachankis, J. E., & Goldfried, M. R. (2006). Social anxiety in young gay men. Journal of Anxiety Disorders, 20, 996 –1015.
Parsons, J. T., VanOra, J., Missildine, W., Purcell, D. W., & Gómez, C. A. (2004). Positive and negative consequences of HIV disclosure among seropositive injection drug users. AIDS Education & Prevention, 16, 459 – 475.
Pennebaker, J. W. (1997). Opening up: The healing power of expressing emotions (Rev. ed.). New York: Guilford Press.
Pennebaker, J. W., Kiecolt-Glaser, J. K., & Glaser, R. (1988). Disclosure of traumas and immune function: Health implications for psychotherapy. Journal of Consulting and Clinical Psychology, 56, 239 –245.
Peterson, J. L., Folkman, S., & Bakeman, R. (1996). Stress, coping, HIV status, psychosocial resources, and depressive mood in African American gay, bisexual, and heterosexual men. American Journal of Community Psychology, 24, 461– 487.
Petronio, S. (2002). Boundaries of privacy: Dialectics of disclosure. Albany: State University of New York Press.
Quinn, D. M., Kahng, S. K., & Crocker, J. (2004). Discreditable: Stigma effects of revealing a mental illness history on test performance. Personality & Social Psychology Bulletin, 30, 803– 815.
- See in Ipce's Library (4) also:
Quinn, Diane M., & Earnshaw Valerie A.; Concealable Stigmatized Identities and Psychological Well-Being; Soc Personal Psychol Compass.; Jan 7(1), 40–51
Remennick, L. (2000). Childless in the land of imperative motherhood: Stigma and coping among infertile Israeli women. Sex Roles, 43, 821–841.
Richards, J. M., Beal, W. E., Seagal, J. D., & Pennebaker, J. W. (2000). Effects of disclosure of traumatic events on illness behavior among psychiatric prison inmates. Journal of Abnormal Psychology, 109, 156–160.
Rintamaki, L. S., & Brashers, D. E. (2005). Social identity and stigma management for people living with HIV. In E. B. Ray (Ed.), Health communication in practice: A case study approach (pp. 145–156). Mahwah, NJ: Erlbaum.
Roemer, L., & Borkovec, T. D. (1993). Worry: Unwanted cognitive activity that controls unwanted somatic experience. In D. M. Wegner & J. W. Pennebaker (Eds.), Handbook of mental control (pp. 220–238). Englewood Cliffs, NJ: Prentice Hall.
Ross, L., & Nisbett, R. E. (1991). The person and the situation. New York: McGraw-Hill.
Safren, S. A., & Pantalone, D. W. (2006). Social anxiety and barriers to resilience among lesbian, gay, and bisexual adolescents. In A. M. Omoto & H. S. Kurtzman (Eds.), Sexual orientation and mental health: Examining identity and development in lesbian, gay, and bisexual people (pp. 55–71). Washington, DC: American Psychological Association.
Salovey, P., & Birnbaum, D. (1989). Influence of mood on health-relevant cognitions. Journal of Personality and Social Psychology, 57, 539 –551.
Sandfort, T. G. M., de Graaf, R., Bijl, R. V., & Schnabel, P. (2001). Same-sex sexual behavior and psychiatric disorders: Findings from the Netherlands mental health survey and incidence study (NEMESIS). Archives of General Psychiatry, 58, 85–91.
Santuzzi, A. M., & Ruscher, J. B. (2002). Stigma salience and paranoid social cognition: Understanding variability in metaperceptions among individuals with recently-acquired stigma. Social Cognition, 20, 171– 197.
Savin-Williams, R. C. (1989). Coming out to parents and self-esteem among gay and lesbian youths. Journal of Homosexuality, 18, 1–35.
Schachter, S., & Singer, J. (1962). Cognitive, social, and physiological determinants of emotional state. Psychological Review, 69, 379 –399.
Schaffer, J. A., & Diamond, R. (1993). Infertility: Private pain and secret stigma. In E. Imber-Black (Ed.), Secrets in families and family therapy (pp. 106–120). New York: Norton.
Shoda, Y., Mischel, W., & Wright, J. C. (1989). Intuitive interactionism in person perception: Effects of situation-behavior relations on dispositional judgments. Journal of Personality and Social Psychology, 56, 41–53.
Simoni, J. M., Mason, H. R. C., Marks, G., Ruiz, M. S., Reed, D., & Richardson, J. L. (1995). Women’s self-disclosure of HIV infection: Rates, reasons, and reactions. Journal of Consulting and Clinical Psychology, 63, 474 – 478.
Smart, L., & Wegner, D. M. (1999). Covering up what can’t be seen: Concealable stigma and mental control. Journal of Personality and Social Psychology, 77, 474 – 486.
Smart, L., & Wegner, D. M. (2000). The hidden costs of hidden stigma. In T. F. Heatherton & R. E. Kleck (Eds.), Social psychology of stigma (pp. 220–242). New York: Guilford Press.
Snyder, M. (1987). Public appearances, private realities: The psychology of self-monitoring. New York: Freeman/Times Books/Holt.
Spielberger, C. D. (1972). Anxiety: Current trends in theory and research. I. New York: Academic Press.
Steele, C. M., Spencer, S. J., & Aronson, J. (2002). Contending with group image: The psychology of stereotype and social identity threat. In M. P. Zanna (Ed.), Advances in experimental social psychology (Vol. 34, pp. 379–440). San Diego, CA: Academic Press.
Stiles, W. B. (1995). Disclosure as a speech act: Is it psychotherapeutic to disclose? In J. W. Pennebaker (Ed.), Emotion, disclosure, & health (pp. 71–91). Washington, DC: American Psychological Association.
Teasdale, J. D., & Russell, M. L. (1983). Differential aspects of induced mood on the recall of positive, negative, and neutral words. British Journal of Clinical Psychology, 22, 163–171.
Ullrich, P. M., Lutgendorf, S. K., & Stapleton, J. T. (2003). Concealment of homosexual identity, social support and CD4 cell count among HIV-seropositive gay men. Journal of Psychosomatic Research, 54, 205–212.
Vohs, K. D., Baumeister, R. F., & Ciarocco, N. J. (2005). Self-regulation and self-presentation: Regulatory resource depletion impairs impression management and effortful self-presentation depletes regulatory resources. Journal of Personality and Social Psychology, 88, 632– 657.
Watters, J. K., & Biernacki, P. (1989). Targeted sampling: Options for the study of hidden populations. Social Problems, 36, 416 – 430.
Wegner, D. M., & Erber, R. (1992). The hyperaccessibility of suppressed thoughts. Journal of Personality and Social Psychology, 63, 903–912.
Wegner, D. M., Erber, R., & Zanakos, S. (1993). Ironic processes in the mental control of mood and mood-related thought. Journal of Personality and Social Psychology, 65, 1093–1104.
Wegner, D. M., & Gold, D. B. (1995). Fanning old flames: Emotional and cognitive effects of suppressing thoughts of a past relationship. Journal of Personality and Social Psychology, 68, 782–792.
Wegner, D. M., & Lane, J. D. (1995). From secrecy to psychopathology. In J. W. Pennebaker (Ed.), Emotion, disclosure, & health (pp. 25–46). Washington, DC: American Psychological Association.
Wegner, D. M., Schneider, D. J., Carter, S. R., & White, T. L. (1987). Paradoxical effects of thought suppression. Journal of Personality and Social Psychology, 53, 5–13.
Wethington, E., & Kessler, R. C. (1986). Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior, 27, 78 – 89.
Whiteford, L. M., & Gonzalez, L. (1995). Stigma: The hidden burden of infertility. Social Science & Medicine, 40, 27–36.
Williams, D. R., Yu, Y., Jackson, J. S., & Anderson, N. B. (1997). Racial differences in physical and mental health: Socioeconomic status, stress and discrimination. American Journal of Health Psychology, 2, 335– 351.
Woods, S. E., & Harbeck, K. M. (1991). Living in two worlds: The identity management strategies used by lesbian physical educators. Journal of Homosexuality, 22, 141–166.
- Received October 26, 2005 Revision received July 17, 2006 Accepted August 11, 2006